
25.2 : Anatomie générale du transport urinaire
- Page ID
- 195290

Objectifs d'apprentissage
- Identifier les uretères, la vessie et l'urètre, ainsi que leur emplacement, leur structure, leur histologie et leur fonction
- Comparez et comparez les urétras masculins et féminins
- Décrivez le réflexe mictionnel
- Décrire le contrôle neuronal volontaire et involontaire de la miction
Plutôt que de commencer par la formation d'urine, cette section débutera par l'excrétion urinaire. L'urine est un liquide de composition variable qui nécessite des structures spécialisées pour l'éliminer de l'organisme de manière sûre et efficace. Le sang est filtré et le filtrat est transformé en urine à un rythme relativement constant tout au long de la journée. Ce liquide traité est conservé jusqu'à un moment opportun pour être excrété. Toutes les structures impliquées dans le transport et le stockage de l'urine sont suffisamment grandes pour être visibles à l'œil nu. Ce système de transport et de stockage ne se contente pas de stocker les déchets, mais il protège les tissus contre les dommages dus à la large gamme de pH et d'osmolarité de l'urine, prévient l'infection par des organismes étrangers et, pour le mâle, assure des fonctions de reproduction.
urètre
L'urètre transporte l'urine de la vessie vers l'extérieur du corps pour y être éliminée. L'urètre est le seul organe urologique qui présente une différence anatomique significative entre les hommes et les femmes ; toutes les autres structures de transport urinaire sont identiques (Figure\(\PageIndex{1}\)).

L'urètre, tant chez l'homme que chez la femme, commence en dessous et au centre des deux ouvertures urétérales qui forment les trois points d'une zone triangulaire à la base de la vessie appelée trigone (grec tri- = « triangle » et racine du mot « trigonométrie »). L'urètre suit les voies postérieure et inférieure à la symphyse pubienne (voir Figure\(\PageIndex{1}\) .a). Chez les mâles et les femelles, l'urètre proximal est tapissé d'un épithélium de transition, tandis que la partie terminale est un épithélium squameux stratifié non kératinisé. Chez le mâle, un épithélium cylindrique pseudostratifié tapisse l'urètre entre ces deux types de cellules. La miction est régulée par un sphincter urinaire interne contrôlé par le système nerveux autonome involontaire, composé de muscles lisses et de muscles squelettiques volontaires qui forment le sphincter urinaire externe situé en dessous.
Urètre féminin
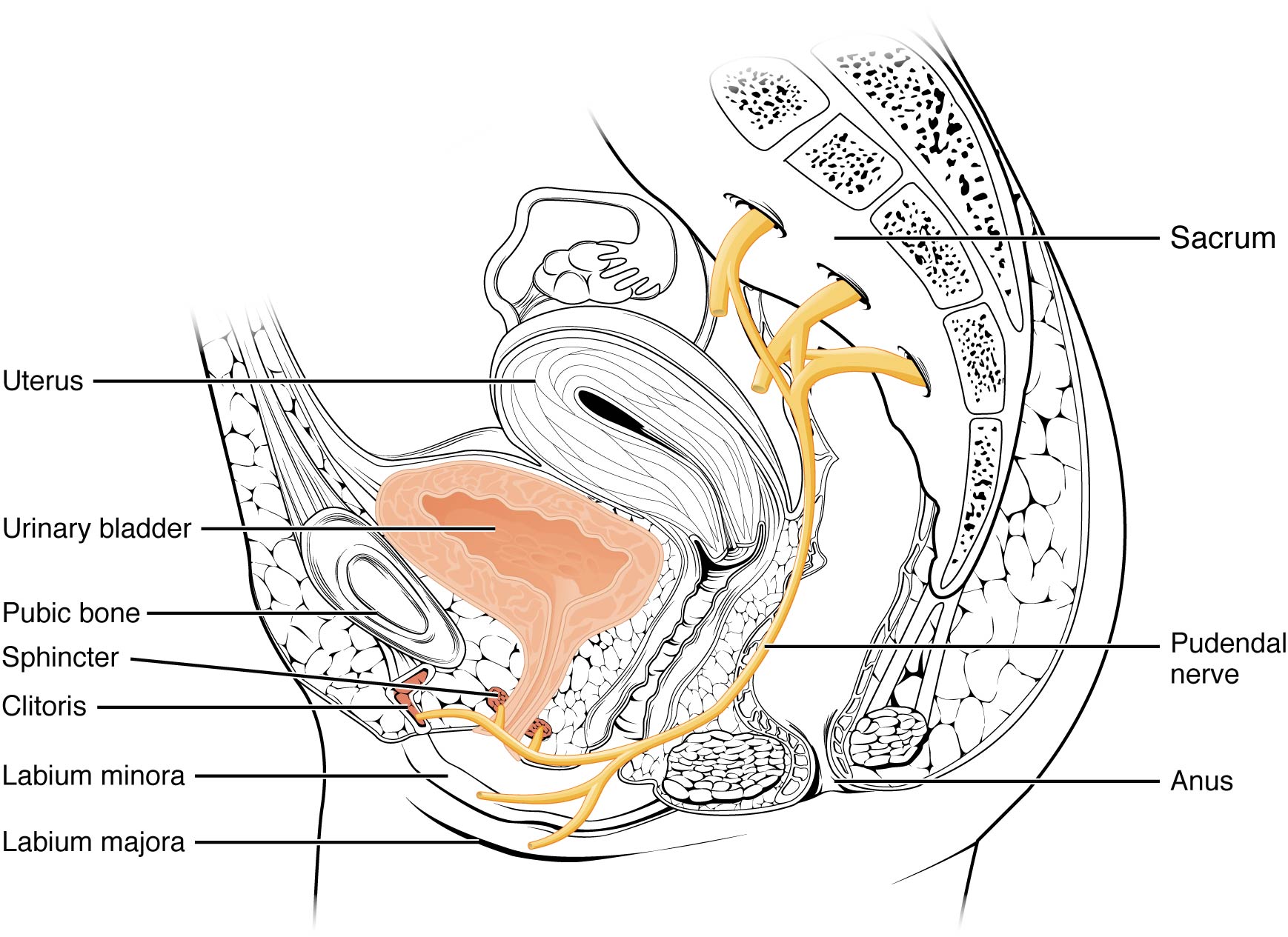
L'orifice urétral externe est encastré dans la paroi vaginale antérieure inférieure au clitoris, au-dessus de l'ouverture vaginale (introïte) et médiale par rapport aux petites lèvres. Sa courte longueur, d'environ 4 cm, constitue moins une barrière contre les bactéries fécales que l'urètre masculin plus long et constitue la meilleure explication de l'incidence plus élevée des infections urinaires chez les femmes. Le contrôle volontaire du sphincter urétral externe est fonction du nerf pudendal. Il apparaît dans la région sacrée de la moelle épinière et se déplace via les nerfs S2—S4 du plexus sacré.
Urètre masculin
L'urètre masculin traverse la prostate juste en dessous de la vessie avant de passer sous la symphyse pubienne (voir Figure\(\PageIndex{1}\) .b). La longueur de l'urètre masculin varie d'un homme à l'autre mais est en moyenne de 20 cm. Il est divisé en quatre régions : l'urètre préprostatique, l'urètre prostatique, l'urètre membraneux et l'urètre spongieux ou pénien. L'urètre préprostatique est très court et intégré à la paroi de la vessie. L'urètre prostatique traverse la prostate. Lors des rapports sexuels, il reçoit le sperme par les canaux éjaculateurs et les sécrétions des vésicules séminales. Deux glandes de Cowper (glandes bulbourétrales) produisent et sécrètent du mucus dans l'urètre pour amortir le pH urétral lors de la stimulation sexuelle. Le mucus neutralise l'environnement habituellement acide et lubrifie l'urètre, diminuant ainsi la résistance à l'éjaculation. L'urètre membraneux traverse les muscles profonds du périnée, où il est investi par les sphincters urétraux sus-jacents. L'urètre spongieux sort à l'extrémité (orifice urétral externe) du pénis après avoir traversé le corps spongieux. Les glandes muqueuses se trouvent sur une grande partie de la longueur de l'urètre et protègent l'urètre des extrêmes du pH urinaire. L'innervation est la même chez les mâles et les femelles.
Vessie
La vessie recueille l'urine des deux uretères (Figure\(\PageIndex{2}\)). La vessie se trouve en avant de l'utérus chez la femme, en arrière de l'os pubien et en avant du rectum. En fin de grossesse, sa capacité est réduite en raison de la compression de l'utérus qui grossit, ce qui entraîne une augmentation de la fréquence des mictions. Chez les hommes, l'anatomie est similaire, sans l'utérus et avec l'ajout de la prostate inférieure à la vessie. La vessie est partiellement rétropéritonéale (à l'extérieur de la cavité péritonéale) et son « dôme » recouvert de péritonéal fait saillie dans l'abdomen lorsque la vessie est distendue par de l'urine.
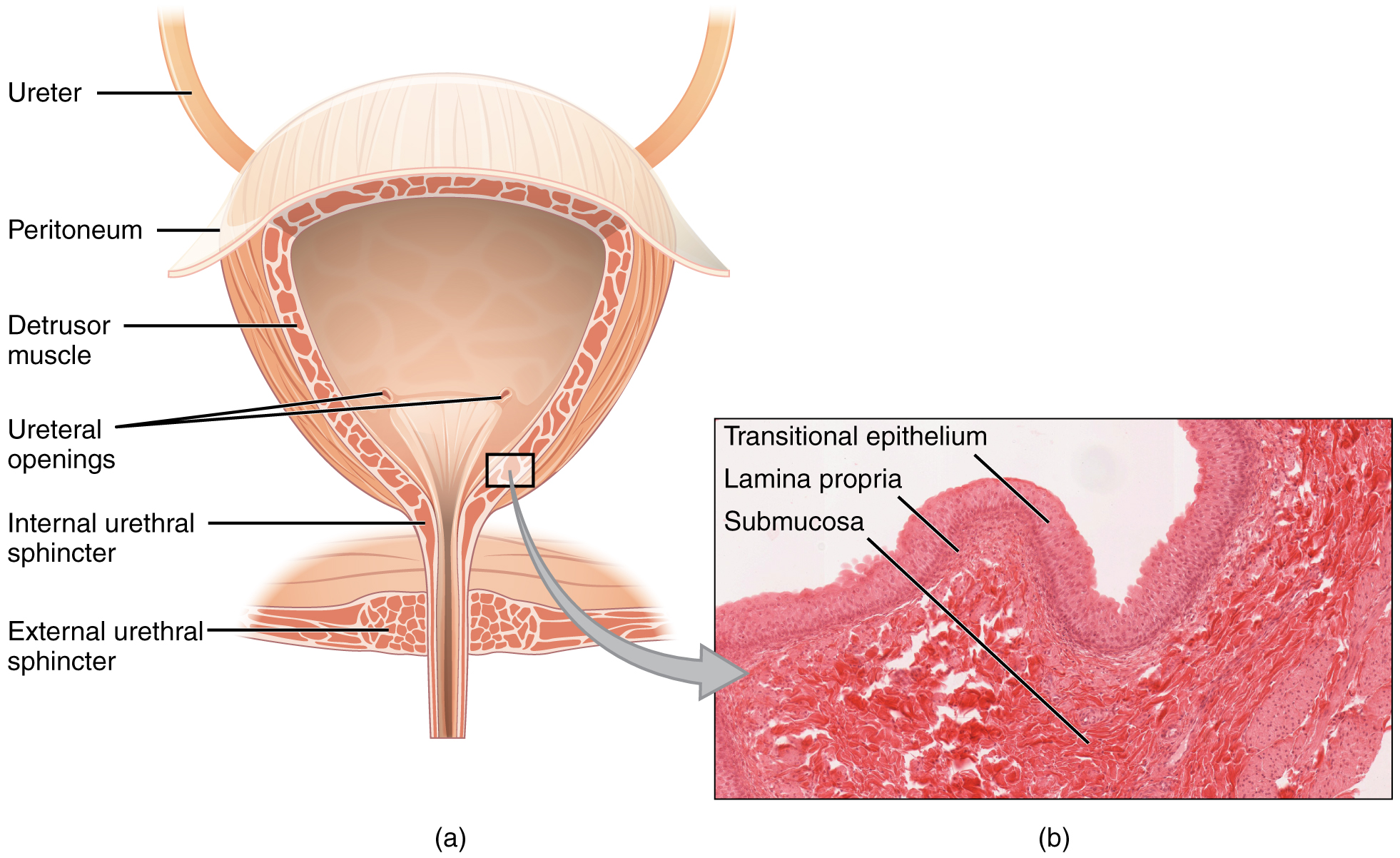

La vessie est un organe hautement distensible composé de bandes irrégulières de muscles lisses qui s'entrecroisent, collectivement appelées muscle détrusor. La surface intérieure est constituée d'un épithélium cellulaire de transition qui est structurellement adapté aux fortes fluctuations de volume de la vessie. Lorsqu'il est vide, il ressemble à un épithélium colonnaire, mais lorsqu'il est étiré, il « passe » (d'où son nom) à une apparence squameuse (voir Figure\(\PageIndex{2}\)). Volumes in adults can range from nearly zero to 500–600 mL.
The detrusor muscle contracts with significant force in the young. The bladder’s strength diminishes with age, but voluntary contractions of abdominal skeletal muscles can increase intra-abdominal pressure to promote more forceful bladder emptying. Such voluntary contraction is also used in forceful defecation and childbirth.
Micturition Reflex
Micturition is a less-often used, but proper term for urination or voiding. It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters. When bladder volume reaches about 150 mL, an urge to void is sensed but is easily overridden. Voluntary control of urination relies on consciously preventing relaxation of the external urethral sphincter to maintain urinary continence. As the bladder fills, subsequent urges become harder to ignore. Ultimately, voluntary constraint fails with resulting incontinence, which will occur as bladder volume approaches 300 to 400 mL.
Normal micturition is a result of stretch receptors in the bladder wall that transmit nerve impulses to the sacral region of the spinal cord to generate a spinal reflex. The resulting parasympathetic neural outflow causes contraction of the detrusor muscle and relaxation of the involuntary internal urethral sphincter. At the same time, the spinal cord inhibits somatic motor neurons, resulting in the relaxation of the skeletal muscle of the external urethral sphincter. The micturition reflex is active in infants but with maturity, children learn to override the reflex by asserting external sphincter control, thereby delaying voiding (potty training). This reflex may be preserved even in the face of spinal cord injury that results in paraplegia or quadriplegia. However, relaxation of the external sphincter may not be possible in all cases, and therefore, periodic catheterization may be necessary for bladder emptying.
Nerves involved in the control of urination include the hypogastric, pelvic, and pudendal (Figure \(\PageIndex{3}\)). Voluntary micturition requires an intact spinal cord and functional pudendal nerve arising from the sacral micturition center. Since the external urinary sphincter is voluntary skeletal muscle, actions by cholinergic neurons maintain contraction (and thereby continence) during filling of the bladder. At the same time, sympathetic nervous activity via the hypogastric nerves suppresses contraction of the detrusor muscle. With further bladder stretch, afferent signals traveling over sacral pelvic nerves activate parasympathetic neurons. This activates efferent neurons to release acetylcholine at the neuromuscular junctions, producing detrusor contraction and bladder emptying.
Ureters
The kidneys and ureters are completely retroperitoneal, and the bladder has a peritoneal covering only over the dome. As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel-shaped renal pelvis in the hilum of each kidney. The hilum narrows to become the ureter of each kidney. As urine passes through the ureter, it does not passively drain into the bladder but rather is propelled by waves of peristalsis. As the ureters enter the pelvis, they sweep laterally, hugging the pelvic walls. As they approach the bladder, they turn medially and pierce the bladder wall obliquely. This is important because it creates an one-way valve (a physiological sphincter rather than an anatomical sphincter) that allows urine into the bladder but prevents reflux of urine from the bladder back into the ureter. Children born lacking this oblique course of the ureter through the bladder wall are susceptible to “vesicoureteral reflux,” which dramatically increases their risk of serious UTI. Pregnancy also increases the likelihood of reflux and UTI.
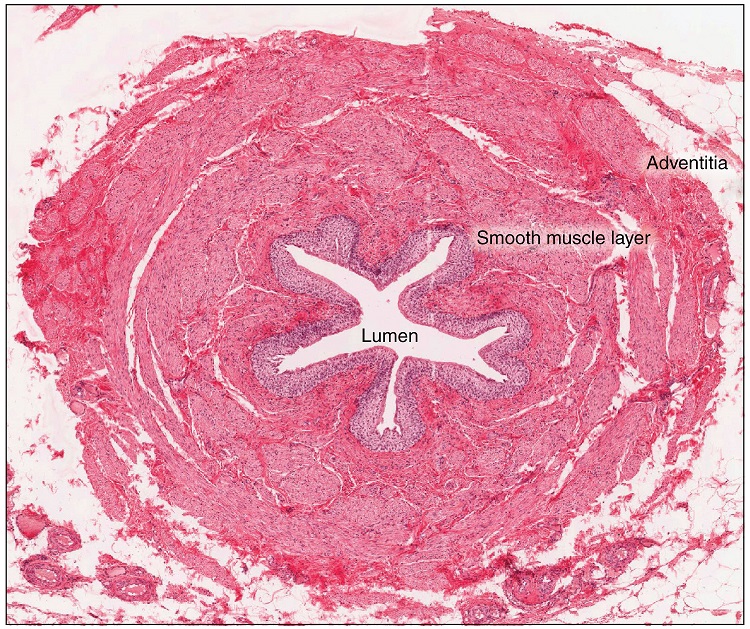
The ureters are approximately 30 cm long. The inner mucosa is lined with transitional epithelium (Figure \(\PageIndex{4}\)) and scattered goblet cells that secrete protective mucus. The muscular layer of the ureter consists of longitudinal and circular smooth muscles that create the peristaltic contractions to move the urine into the bladder without the aid of gravity. Finally, a loose adventitial layer composed of collagen and fat anchors the ureters between the parietal peritoneum and the posterior abdominal wall.
Chapter Review
The urethra is the only urinary structure that differs significantly between males and females. This is due to the dual role of the male urethra in transporting both urine and semen. The urethra arises from the trigone area at the base of the bladder. Urination is controlled by an involuntary internal sphincter of smooth muscle and a voluntary external sphincter of skeletal muscle. The shorter female urethra contributes to the higher incidence of bladder infections in females. The male urethra receives secretions from the prostate gland, Cowper’s gland, and seminal vesicles as well as sperm. The bladder is largely retroperitoneal and can hold up to 500–600 mL urine. Micturition is the process of voiding the urine and involves both involuntary and voluntary actions. Voluntary control of micturition requires a mature and intact sacral micturition center. It also requires an intact spinal cord. Loss of control of micturition is called incontinence and results in voiding when the bladder contains about 250 mL urine. The ureters are retroperitoneal and lead from the renal pelvis of the kidney to the trigone area at the base of the bladder. A thick muscular wall consisting of longitudinal and circular smooth muscle helps move urine toward the bladder by way of peristaltic contractions.
Review Questions
Q. Peristaltic contractions occur in the ________.
A. urethra
B. bladder
C. ureters
D. urethra, bladder, and ureters
Answer: C
Q. Somatic motor neurons must be ________ to relax the external urethral sphincter to allow urination.
A. stimulated
B. inhibited
Answer: B
Q. Which part of the urinary system is not completely retroperitoneal?
A. kidneys
B. ureters
C. bladder
D. nephrons
Answer: C
Critical Thinking Questions
Q. Why are females more likely to contract bladder infections than males?
A. The longer urethra of males means bacteria must travel farther to the bladder to cause an infection.
Q. Describe how forceful urination is accomplished.
A. Forceful urination is accomplished by contraction of abdominal muscles.
Glossary
- anatomical sphincter
- smooth or skeletal muscle surrounding the lumen of a vessel or hollow organ that can restrict flow when contracted
- detrusor muscle
- smooth muscle in the bladder wall; fibers run in all directions to reduce the size of the organ when emptying it of urine
- external urinary sphincter
- skeletal muscle; must be relaxed consciously to void urine
- internal urinary sphincter
- smooth muscle at the juncture of the bladder and urethra; relaxes as the bladder fills to allow urine into the urethra
- incontinence
- loss of ability to control micturition
- micturition
- also called urination or voiding
- physiological sphincter
- sphincter consisting of circular smooth muscle indistinguishable from adjacent muscle but possessing differential innervations, permitting its function as a sphincter; structurally weak
- retroperitoneal
- outside the peritoneal cavity; in the case of the kidney and ureters, between the parietal peritoneum and the abdominal wall
- sacral micturition center
- group of neurons in the sacral region of the spinal cord that controls urination; acts reflexively unless its action is modified by higher brain centers to allow voluntary urination
- trigone
- area at the base of the bladder marked by the two ureters in the posterior–lateral aspect and the urethral orifice in the anterior aspect oriented like points on a triangle
- urethra
- transports urine from the bladder to the outside environment