
25.2: التشريح الإجمالي لنقل البول
- Page ID
- 203195

أهداف التعلم
- حدد الحالب والمثانة البولية والإحليل، بالإضافة إلى موقعها وهيكلها وأنسجها ووظيفتها
- قارن وقارن بين الإحليل الذكري والأنثوي
- وصف منعكس التبول
- وصف التحكم العصبي الطوعي وغير الطوعي في التبول
بدلاً من البدء بتكوين البول، سيبدأ هذا القسم بإفراز البول. البول هو سائل ذو تركيبة متغيرة يتطلب هياكل متخصصة لإزالته من الجسم بأمان وكفاءة. يتم تصفية الدم، ويتم تحويل المرشح إلى بول بمعدل ثابت نسبيًا على مدار اليوم. يتم تخزين هذا السائل المعالج حتى وقت مناسب للإفراز. جميع الهياكل المشاركة في نقل وتخزين البول كبيرة بما يكفي لتكون مرئية للعين المجردة. لا يقوم نظام النقل والتخزين هذا بتخزين النفايات فحسب، بل يحمي الأنسجة من التلف بسبب النطاق الواسع لدرجة الحموضة وأسمولية البول، ويمنع العدوى بالكائنات الحية الغريبة، وبالنسبة للذكور، يوفر وظائف الإنجاب.
إحليل
يقوم مجرى البول بنقل البول من المثانة إلى خارج الجسم للتخلص منه. الإحليل هو العضو البولي الوحيد الذي يظهر أي فرق تشريحي كبير بين الذكور والإناث؛ جميع هياكل نقل البول الأخرى متطابقة (الشكل\(\PageIndex{1}\)).

يبدأ مجرى البول في كل من الذكور والإناث في الأسفل والمركزي من فتحتي الحالب، مما يشكل النقاط الثلاث لمنطقة على شكل مثلث عند قاعدة المثانة تسمى المثلث (اليونانية ثلاثية = «المثلث» وجذر كلمة «علم المثلثات»). يتتبع مجرى البول الجزء الخلفي والسفلي من ارتفاق العانة (انظر الشكل\(\PageIndex{1}\) أ.). في كل من الذكور والإناث، يُبطن مجرى البول القريب ظهارة انتقالية، في حين أن الجزء الطرفي هو ظهارة حرشفية طبقية غير كيراتينية. في الذكور، تبطن الظهارة العمودية الكاذبة مجرى البول بين هذين النوعين من الخلايا. يتم تنظيم الإفراغ عن طريق العضلة العاصرة البولية الداخلية التي يتحكم فيها الجهاز العصبي اللاإرادي، والتي تتكون من العضلات الملساء والعضلات الهيكلية الإرادية التي تشكل العضلة العاصرة البولية الخارجية تحتها.
مجرى البول الأنثوي
يتم تضمين فتحة مجرى البول الخارجية في جدار المهبل الأمامي السفلي من البظر، وأعلى من فتحة المهبل (الأمعاء)، ووسطي إلى الشفرين الصغيرين. يعد طوله القصير، حوالي 4 سم، أقل عائقًا للبكتيريا البرازية من مجرى البول الذكري الأطول وأفضل تفسير لزيادة حدوث عدوى المسالك البولية لدى النساء. السيطرة الطوعية على العضلة العاصرة الإحليلية الخارجية هي وظيفة للعصب الفرجي. ينشأ في المنطقة العجزية من الحبل الشوكي، وينتقل عبر أعصاب S2-S4 للضفيرة العجزية.
إحليل الذكور
يمر مجرى البول الذكري عبر غدة البروستاتا مباشرة أسفل المثانة قبل أن يمر أسفل ارتفاق العانة (انظر الشكل\(\PageIndex{1}\) ب). يختلف طول مجرى البول الذكري بين الرجال ولكنه يبلغ في المتوسط 20 سم في الطول. ينقسم إلى أربع مناطق: مجرى البول قبل البروستاتا، والإحليل البروستاتي، والإحليل الغشائي، والإحليل الإسفنجي أو القضيبي. مجرى البول قبل البروستاتا قصير جدًا ويتم دمجه في جدار المثانة. يمر مجرى البول البروستاتي عبر غدة البروستاتا. أثناء الجماع، تستقبل الحيوانات المنوية عبر قنوات القذف والإفرازات من الحويصلات المنوية. تنتج غدد كوبر المزدوجة (الغدد البصلية الإحليلية) المخاط وتفرزه في مجرى البول للحد من درجة حموضة الإحليل أثناء التحفيز الجنسي. يعمل المخاط على تحييد البيئة الحمضية المعتادة وتزييت مجرى البول، مما يقلل من مقاومة القذف. يمر مجرى البول الغشائي عبر العضلات العميقة للعجان، حيث يتم استثماره بواسطة العضلة العاصرة للإحليل المغطية. يخرج مجرى البول الإسفنجي عند طرف القضيب (فتحة الإحليل الخارجية) بعد المرور عبر الجسم الإسفنجي. توجد الغدد المخاطية على طول جزء كبير من مجرى البول وتحمي مجرى البول من أقصى درجات الحموضة في البول. التعصيب هو نفسه في كل من الذكور والإناث.
مثانة
تجمع المثانة البولية البول من كلا الحالب (الشكل\(\PageIndex{2}\)). تقع المثانة أمام الرحم عند الإناث، خلف عظمة العانة وأمام المستقيم. في أواخر الحمل، تنخفض قدرتها بسبب الضغط عن طريق الرحم المتضخم، مما يؤدي إلى زيادة وتيرة التبول. في الذكور، يكون التشريح مشابهًا، باستثناء الرحم، ومع إضافة البروستاتا السفلية للمثانة. تتكون المثانة جزئيًا من خلف الصفاق (خارج التجويف البريتوني) مع ظهور «القبة» المغطاة بالصفاق في البطن عندما تنتفخ المثانة بالبول.
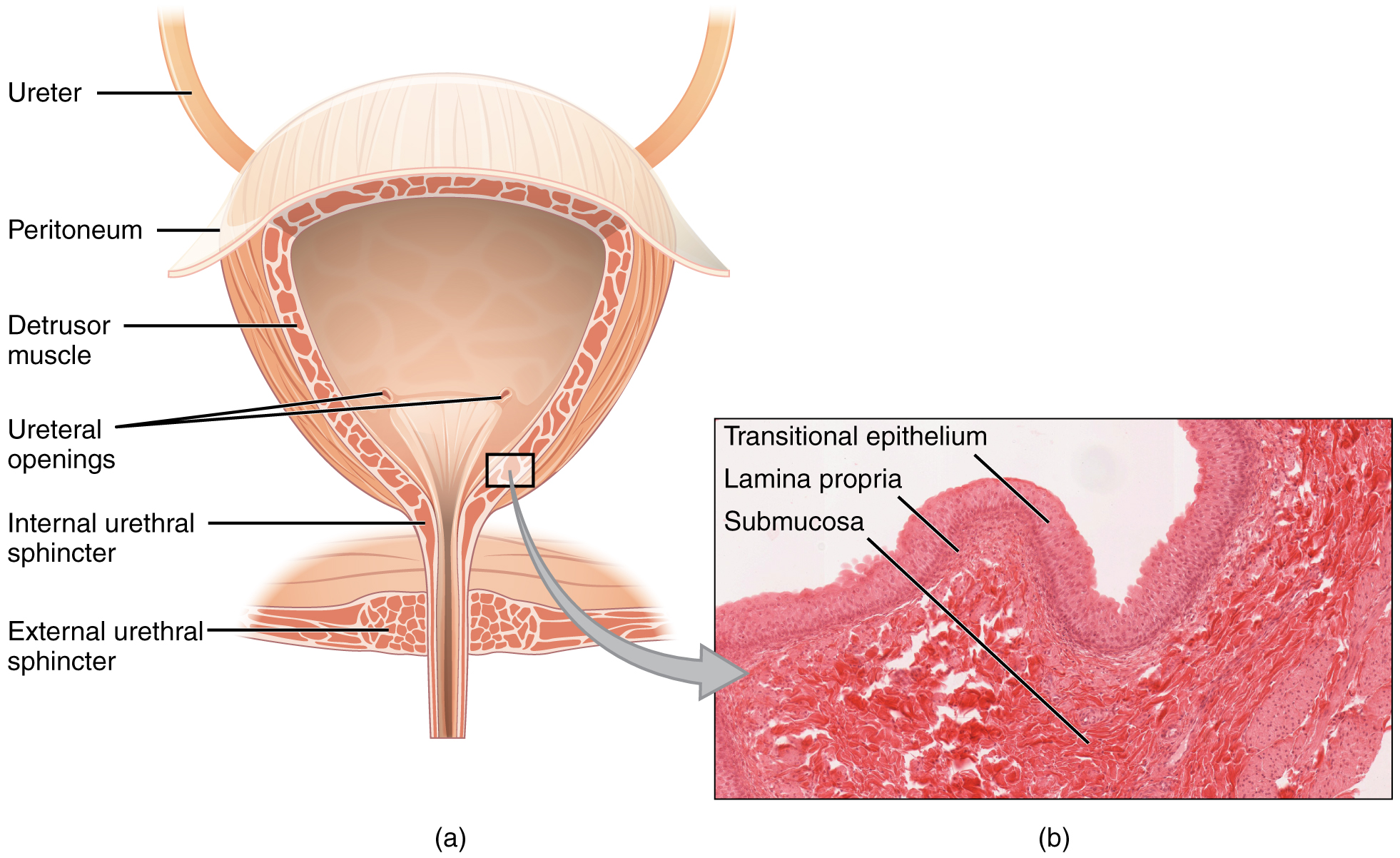

المثانة عبارة عن عضو شديد الإنتفاخ يتكون من أشرطة متقاطعة غير منتظمة من العضلات الملساء تسمى مجتمعة العضلة الضادة. يتكون السطح الداخلي من ظهارة خلوية انتقالية مناسبة هيكليًا لتقلبات الحجم الكبيرة للمثانة. عندما تكون فارغة، فإنها تشبه الظهارة العمودية، ولكن عندما تتمدد، فإنها «تنتقل» (ومن هنا جاءت تسميتها) إلى مظهر حرشفي (انظر الشكل)\(\PageIndex{2}\)). Volumes in adults can range from nearly zero to 500–600 mL.
The detrusor muscle contracts with significant force in the young. The bladder’s strength diminishes with age, but voluntary contractions of abdominal skeletal muscles can increase intra-abdominal pressure to promote more forceful bladder emptying. Such voluntary contraction is also used in forceful defecation and childbirth.
Micturition Reflex
Micturition is a less-often used, but proper term for urination or voiding. It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters. When bladder volume reaches about 150 mL, an urge to void is sensed but is easily overridden. Voluntary control of urination relies on consciously preventing relaxation of the external urethral sphincter to maintain urinary continence. As the bladder fills, subsequent urges become harder to ignore. Ultimately, voluntary constraint fails with resulting incontinence, which will occur as bladder volume approaches 300 to 400 mL.
Normal micturition is a result of stretch receptors in the bladder wall that transmit nerve impulses to the sacral region of the spinal cord to generate a spinal reflex. The resulting parasympathetic neural outflow causes contraction of the detrusor muscle and relaxation of the involuntary internal urethral sphincter. At the same time, the spinal cord inhibits somatic motor neurons, resulting in the relaxation of the skeletal muscle of the external urethral sphincter. The micturition reflex is active in infants but with maturity, children learn to override the reflex by asserting external sphincter control, thereby delaying voiding (potty training). This reflex may be preserved even in the face of spinal cord injury that results in paraplegia or quadriplegia. However, relaxation of the external sphincter may not be possible in all cases, and therefore, periodic catheterization may be necessary for bladder emptying.
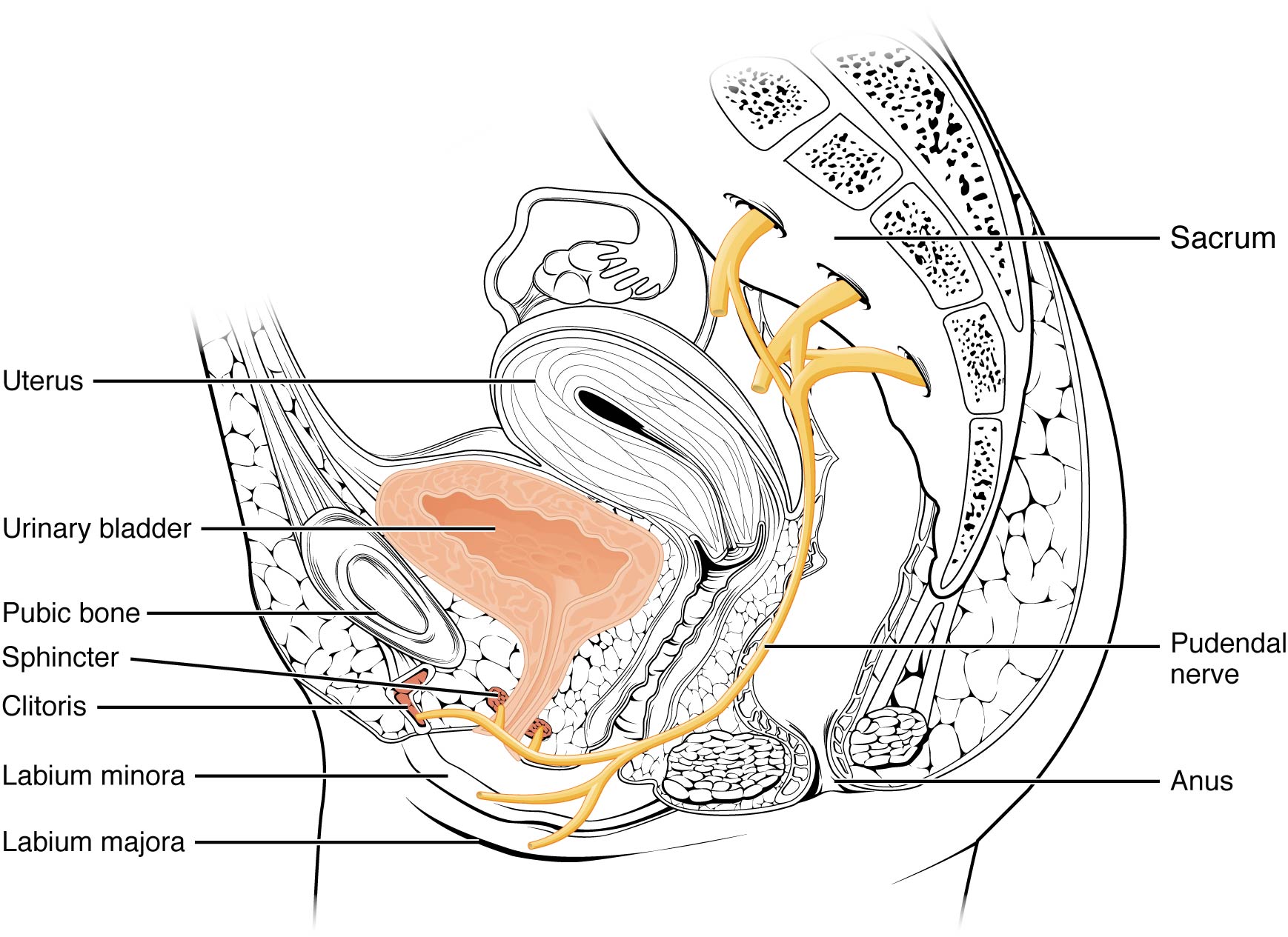
Nerves involved in the control of urination include the hypogastric, pelvic, and pudendal (Figure \(\PageIndex{3}\)). Voluntary micturition requires an intact spinal cord and functional pudendal nerve arising from the sacral micturition center. Since the external urinary sphincter is voluntary skeletal muscle, actions by cholinergic neurons maintain contraction (and thereby continence) during filling of the bladder. At the same time, sympathetic nervous activity via the hypogastric nerves suppresses contraction of the detrusor muscle. With further bladder stretch, afferent signals traveling over sacral pelvic nerves activate parasympathetic neurons. This activates efferent neurons to release acetylcholine at the neuromuscular junctions, producing detrusor contraction and bladder emptying.
Ureters
The kidneys and ureters are completely retroperitoneal, and the bladder has a peritoneal covering only over the dome. As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel-shaped renal pelvis in the hilum of each kidney. The hilum narrows to become the ureter of each kidney. As urine passes through the ureter, it does not passively drain into the bladder but rather is propelled by waves of peristalsis. As the ureters enter the pelvis, they sweep laterally, hugging the pelvic walls. As they approach the bladder, they turn medially and pierce the bladder wall obliquely. This is important because it creates an one-way valve (a physiological sphincter rather than an anatomical sphincter) that allows urine into the bladder but prevents reflux of urine from the bladder back into the ureter. Children born lacking this oblique course of the ureter through the bladder wall are susceptible to “vesicoureteral reflux,” which dramatically increases their risk of serious UTI. Pregnancy also increases the likelihood of reflux and UTI.
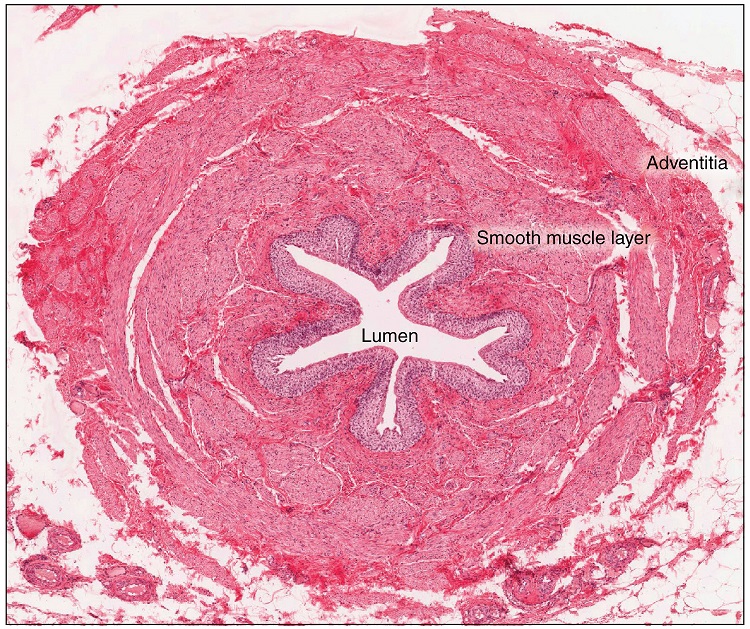
The ureters are approximately 30 cm long. The inner mucosa is lined with transitional epithelium (Figure \(\PageIndex{4}\)) and scattered goblet cells that secrete protective mucus. The muscular layer of the ureter consists of longitudinal and circular smooth muscles that create the peristaltic contractions to move the urine into the bladder without the aid of gravity. Finally, a loose adventitial layer composed of collagen and fat anchors the ureters between the parietal peritoneum and the posterior abdominal wall.
Chapter Review
The urethra is the only urinary structure that differs significantly between males and females. This is due to the dual role of the male urethra in transporting both urine and semen. The urethra arises from the trigone area at the base of the bladder. Urination is controlled by an involuntary internal sphincter of smooth muscle and a voluntary external sphincter of skeletal muscle. The shorter female urethra contributes to the higher incidence of bladder infections in females. The male urethra receives secretions from the prostate gland, Cowper’s gland, and seminal vesicles as well as sperm. The bladder is largely retroperitoneal and can hold up to 500–600 mL urine. Micturition is the process of voiding the urine and involves both involuntary and voluntary actions. Voluntary control of micturition requires a mature and intact sacral micturition center. It also requires an intact spinal cord. Loss of control of micturition is called incontinence and results in voiding when the bladder contains about 250 mL urine. The ureters are retroperitoneal and lead from the renal pelvis of the kidney to the trigone area at the base of the bladder. A thick muscular wall consisting of longitudinal and circular smooth muscle helps move urine toward the bladder by way of peristaltic contractions.
Review Questions
Q. Peristaltic contractions occur in the ________.
A. urethra
B. bladder
C. ureters
D. urethra, bladder, and ureters
Answer: C
Q. Somatic motor neurons must be ________ to relax the external urethral sphincter to allow urination.
A. stimulated
B. inhibited
Answer: B
Q. Which part of the urinary system is not completely retroperitoneal?
A. kidneys
B. ureters
C. bladder
D. nephrons
Answer: C
Critical Thinking Questions
Q. Why are females more likely to contract bladder infections than males?
A. The longer urethra of males means bacteria must travel farther to the bladder to cause an infection.
Q. Describe how forceful urination is accomplished.
A. Forceful urination is accomplished by contraction of abdominal muscles.
Glossary
- anatomical sphincter
- smooth or skeletal muscle surrounding the lumen of a vessel or hollow organ that can restrict flow when contracted
- detrusor muscle
- smooth muscle in the bladder wall; fibers run in all directions to reduce the size of the organ when emptying it of urine
- external urinary sphincter
- skeletal muscle; must be relaxed consciously to void urine
- internal urinary sphincter
- smooth muscle at the juncture of the bladder and urethra; relaxes as the bladder fills to allow urine into the urethra
- incontinence
- loss of ability to control micturition
- micturition
- also called urination or voiding
- physiological sphincter
- sphincter consisting of circular smooth muscle indistinguishable from adjacent muscle but possessing differential innervations, permitting its function as a sphincter; structurally weak
- retroperitoneal
- outside the peritoneal cavity; in the case of the kidney and ureters, between the parietal peritoneum and the abdominal wall
- sacral micturition center
- group of neurons in the sacral region of the spinal cord that controls urination; acts reflexively unless its action is modified by higher brain centers to allow voluntary urination
- trigone
- area at the base of the bladder marked by the two ureters in the posterior–lateral aspect and the urethral orifice in the anterior aspect oriented like points on a triangle
- urethra
- transports urine from the bladder to the outside environment