
19.1: تشريح القلب
- Page ID
- 203265

أهداف التعلم
- وصف موقع وموضع القلب داخل تجويف الجسم
- وصف التشريح الداخلي والخارجي للقلب
- التعرف على طبقات أنسجة القلب
- اربط بنية القلب بوظيفته كمضخة
- قارن الدورة الدموية الجهازية بالدورة الدموية الرئوية
- التعرف على الأوردة والشرايين في نظام الدورة الدموية التاجية
- تتبع مسار الدم المؤكسج وغير المؤكسج في غرف القلب
الأهمية الحيوية للقلب واضحة. إذا افترض المرء أن متوسط معدل الانكماش يبلغ 75 انقباضًا في الدقيقة، فسوف ينقبض قلب الإنسان حوالي 108000 مرة في يوم واحد، وأكثر من 39 مليون مرة في عام واحد، وما يقرب من 3 مليارات مرة خلال عمر 75 عامًا. تقوم كل غرفة من غرف الضخ الرئيسية للقلب بإخراج ما يقرب من 70 مل من الدم لكل انقباض لدى شخص بالغ يستريح. سيكون هذا يساوي 5.25 لترًا من السوائل في الدقيقة وحوالي 14000 لتر في اليوم. على مدى عام واحد، سيعادل ذلك 10,000,000 لتر أو 2.6 مليون جالون من الدم الذي يتم إرساله عبر ما يقرب من 60,000 ميل من الأوعية. من أجل فهم كيفية حدوث ذلك، من الضروري فهم علم التشريح وعلم وظائف الأعضاء في القلب.
موقع القلب
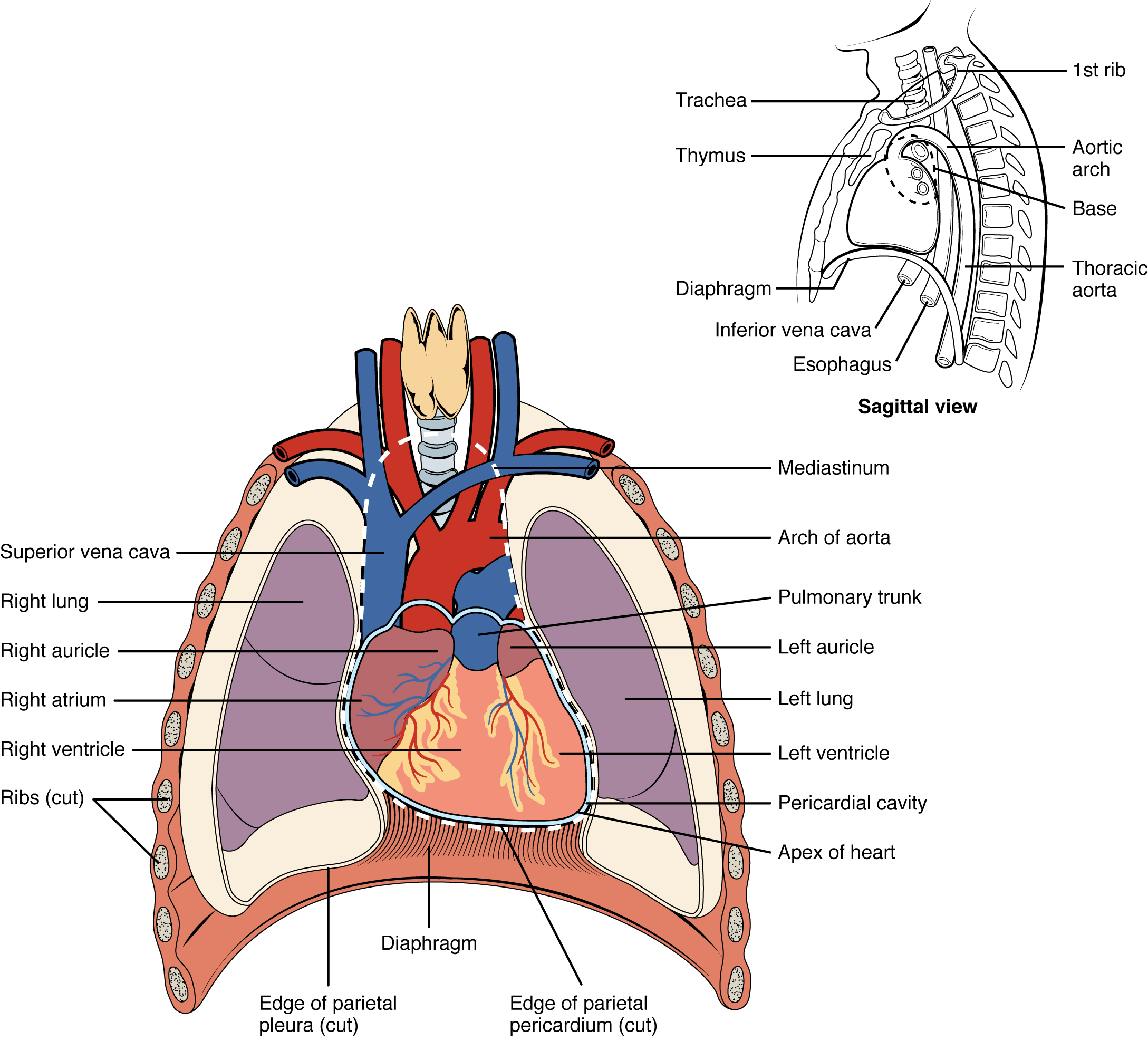
يقع قلب الإنسان داخل التجويف الصدري، بشكل وسطي بين الرئتين في الفضاء المعروف باسم المنصف. \(\PageIndex{1}\)يوضح الشكل موضع القلب داخل التجويف الصدري. داخل المنصف، يتم فصل القلب عن الهياكل المنصفية الأخرى بواسطة غشاء صلب يعرف باسم التامور، أو كيس التامور، ويجلس في مساحته الخاصة التي تسمى تجويف التامور. يقع السطح الظهري للقلب بالقرب من أجسام الفقرات، ويقع سطحه الأمامي في عمق عظمة القص والغضاريف الضلعية. ترتبط الأوردة الكبيرة والأوردة العلوية والسفلية والشرايين الكبيرة والشريان الأورطي والجذع الرئوي بالسطح العلوي للقلب الذي يُطلق عليه القاعدة. تقع قاعدة القلب على مستوى الغضروف الضلعي الثالث، كما هو موضح في الشكل\(\PageIndex{1}\). يقع الطرف السفلي للقلب، وهو القمة، على يسار القص مباشرة بين تقاطع الضلعين الرابع والخامس بالقرب من مفصلهما مع الغضاريف الساحلية. ينحرف الجانب الأيمن من القلب من الأمام، وينحرف الجانب الأيسر للخلف. من المهم تذكر موضع القلب واتجاهه عند وضع سماعة الطبيب على صدر المريض والاستماع إلى أصوات القلب، وكذلك عند النظر إلى الصور الملتقطة من منظور منتصف القوس. ينعكس الانحراف الطفيف للقمة إلى اليسار في انخفاض في السطح الإنسي للفص السفلي للرئة اليسرى، والذي يسمى الشق القلبي.
الاتصال اليومي: CPR
يسمح وضع القلب في الجذع بين الفقرات والقص (انظر الشكل\(\PageIndex{2}\) الخاص بوضع القلب داخل الصدر) للأفراد بتطبيق تقنية الطوارئ المعروفة باسم الإنعاش القلبي الرئوي (CPR) إذا توقف قلب المريض. من خلال الضغط على الجزء المسطح من إحدى اليدين على القص في المنطقة الواقعة بين الخط عند T4 و T9 (الشكل\(\PageIndex{2}\):)، يمكن ضغط الدم يدويًا داخل القلب بما يكفي لدفع بعض الدم بداخله إلى الدوائر الرئوية والجهازية. هذا أمر بالغ الأهمية للدماغ، حيث يحدث تلف لا رجعة فيه وموت الخلايا العصبية في غضون دقائق من فقدان تدفق الدم. تدعو المعايير الحالية إلى ضغط الصدر بعمق 5 سم على الأقل وبمعدل 100 ضغطة في الدقيقة، وهو معدل يساوي النبض في «Staying Alive»، الذي سجلته Bee Gees عام 1977. إذا لم تكن على دراية بهذه الأغنية، يتوفر إصدار على www.youtube.com. في هذه المرحلة، يتم التركيز على إجراء عمليات ضغط عالية الجودة على الصدر، بدلاً من توفير التنفس الصناعي. يتم إجراء الإنعاش القلبي الرئوي بشكل عام حتى يستعيد المريض الانقباض التلقائي أو يتم إعلان وفاته من قبل أخصائي رعاية صحية ذي خبرة.

عند إجراء الإنعاش القلبي الرئوي من قبل أفراد غير مدربين أو متحمسين للغاية، يمكن أن يؤدي الإنعاش القلبي الرئوي إلى كسر الأضلاع أو كسر القص، ويمكن أن يلحق أضرارًا جسيمة إضافية بالمريض. من الممكن أيضًا، إذا تم وضع اليدين في وضع منخفض جدًا على القص، دفع عملية الخزامي يدويًا إلى الكبد، وهي نتيجة قد تكون قاتلة للمريض. التدريب المناسب ضروري. تعتبر هذه التقنية التي أثبتت جدواها في الحفاظ على الحياة ذات قيمة كبيرة لدرجة أنه يجب اعتماد جميع العاملين الطبيين تقريبًا وكذلك الأفراد المعنيين من الجمهور وإعادة اعتمادهم بشكل روتيني في تطبيقها. يتم تقديم دورات CPR في مجموعة متنوعة من المواقع، بما في ذلك الكليات والمستشفيات والصليب الأحمر الأمريكي وبعض الشركات التجارية. عادة ما تتضمن ممارسة تقنية الضغط على عارضة أزياء.

قم بزيارة موقع American Heart Association للمساعدة في تحديد موقع دورة بالقرب من منزلك في الولايات المتحدة. هناك أيضًا العديد من جمعيات القلب الوطنية والإقليمية الأخرى التي تقدم نفس الخدمة، اعتمادًا على الموقع.
شكل وحجم القلب
شكل القلب يشبه كوز الصنوبر، وهو واسع نوعًا ما على السطح العلوي ويتناقص حتى القمة (الشكل 1)\(\PageIndex{1}\)). A typical heart is approximately the size of your fist: 12 cm (5 in) in length, 8 cm (3.5 in) wide, and 6 cm (2.5 in) in thickness. Given the size difference between most members of the sexes, the weight of a female heart is approximately 250–300 grams (9 to 11 ounces), and the weight of a male heart is approximately 300–350 grams (11 to 12 ounces). The heart of a well-trained athlete, especially one specializing in aerobic sports, can be considerably larger than this. Cardiac muscle responds to exercise in a manner similar to that of skeletal muscle. That is, exercise results in the addition of protein myofilaments that increase the size of the individual cells without increasing their numbers, a concept called hypertrophy. Hearts of athletes can pump blood more effectively at lower rates than those of nonathletes. Enlarged hearts are not always a result of exercise; they can result from pathologies, such as hypertrophic cardiomyopathy. The cause of an abnormally enlarged heart muscle is unknown, but the condition is often undiagnosed and can cause sudden death in apparently otherwise healthy young people.
Chambers and Circulation through the Heart
The human heart consists of four chambers: The left side and the right side each have one atrium and one ventricle. Each of the upper chambers, the right atrium (plural = atria) and the left atrium, acts as a receiving chamber and contracts to push blood into the lower chambers, the right ventricle and the left ventricle. The ventricles serve as the primary pumping chambers of the heart, propelling blood to the lungs or to the rest of the body.
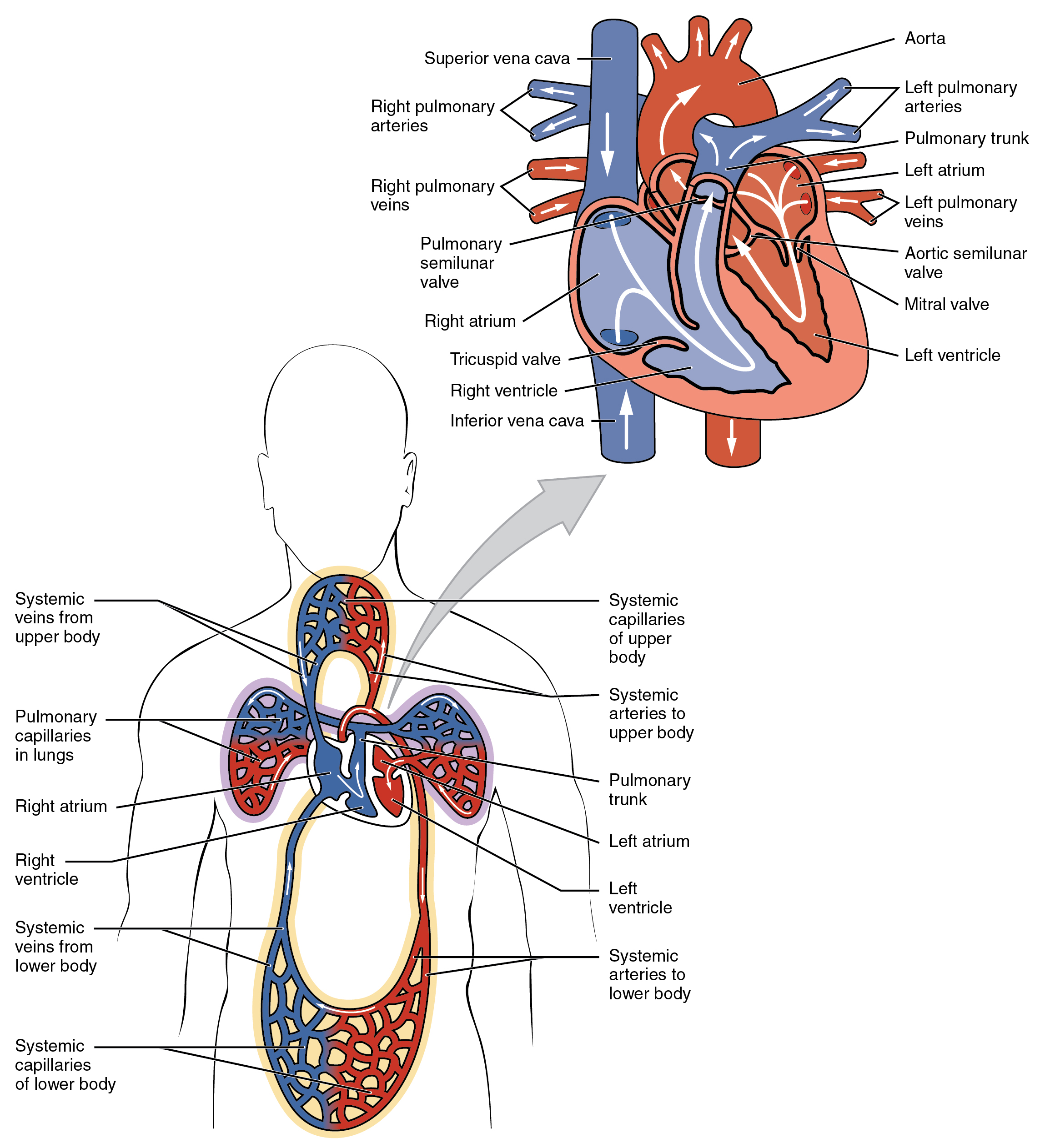
There are two distinct but linked circuits in the human circulation called the pulmonary and systemic circuits. Although both circuits transport blood and everything it carries, we can initially view the circuits from the point of view of gases. The pulmonary circuit transports blood to and from the lungs, where it picks up oxygen and delivers carbon dioxide for exhalation. The systemic circuit transports oxygenated blood to virtually all of the tissues of the body and returns relatively deoxygenated blood and carbon dioxide to the heart to be sent back to the pulmonary circulation.
The right ventricle pumps deoxygenated blood into the pulmonary trunk, which leads toward the lungs and bifurcates into the left and right pulmonary arteries. These vessels in turn branch many times before reaching the pulmonary capillaries, where gas exchange occurs: Carbon dioxide exits the blood and oxygen enters. The pulmonary trunk arteries and their branches are the only arteries in the post-natal body that carry relatively deoxygenated blood. Highly oxygenated blood returning from the pulmonary capillaries in the lungs passes through a series of vessels that join together to form the pulmonary veins—the only post-natal veins in the body that carry highly oxygenated blood. The pulmonary veins conduct blood into the left atrium, which pumps the blood into the left ventricle, which in turn pumps oxygenated blood into the aorta and on to the many branches of the systemic circuit. Eventually, these vessels will lead to the systemic capillaries, where exchange with the tissue fluid and cells of the body occurs. In this case, oxygen and nutrients exit the systemic capillaries to be used by the cells in their metabolic processes, and carbon dioxide and waste products will enter the blood.
The blood exiting the systemic capillaries is lower in oxygen concentration than when it entered. The capillaries will ultimately unite to form venules, joining to form ever-larger veins, eventually flowing into the two major systemic veins, the superior vena cava and the inferior vena cava, which return blood to the right atrium. The blood in the superior and inferior venae cavae flows into the right atrium, which pumps blood into the right ventricle. This process of blood circulation continues as long as the individual remains alive. Understanding the flow of blood through the pulmonary and systemic circuits is critical to all health professions (Figure \(\PageIndex{3}\)).
Membranes, Surface Features, and Layers
Our exploration of more in-depth heart structures begins by examining the membrane that surrounds the heart, the prominent surface features of the heart, and the layers that form the wall of the heart. Each of these components plays its own unique role in terms of function.
Membranes
The membrane that directly surrounds the heart and defines the pericardial cavity is called the pericardium or pericardial sac. It also surrounds the “roots” of the major vessels, or the areas of closest proximity to the heart. The pericardium, which literally translates as “around the heart,” consists of two distinct sublayers: the sturdy outer fibrous pericardium and the inner serous pericardium. The fibrous pericardium is made of tough, dense connective tissue that protects the heart and maintains its position in the thorax. The more delicate serous pericardium consists of two layers: the parietal pericardium, which is fused to the fibrous pericardium, and an inner visceral pericardium, or epicardium, which is fused to the heart and is part of the heart wall. The pericardial cavity, filled with lubricating serous fluid, lies between the epicardium and the pericardium.
In most organs within the body, visceral serous membranes such as the epicardium are microscopic. However, in the case of the heart, it is not a microscopic layer but rather a macroscopic layer, consisting of a simple squamous epithelium called a mesothelium, reinforced with loose, irregular, or areolar connective tissue that attaches to the pericardium. This mesothelium secretes the lubricating serous fluid that fills the pericardial cavity and reduces friction as the heart contracts. Figure \(\PageIndex{4}\) illustrates the pericardial membrane and the layers of the heart.

DISORDERS OF THE ... Heart: Cardiac Tamponade
If excess fluid builds within the pericardial space, it can lead to a condition called cardiac tamponade, or pericardial tamponade. With each contraction of the heart, more fluid—in most instances, blood—accumulates within the pericardial cavity. In order to fill with blood for the next contraction, the heart must relax. However, the excess fluid in the pericardial cavity puts pressure on the heart and prevents full relaxation, so the chambers within the heart contain slightly less blood as they begin each heart cycle. Over time, less and less blood is ejected from the heart. If the fluid builds up slowly, as in hypothyroidism, the pericardial cavity may be able to expand gradually to accommodate this extra volume. Some cases of fluid in excess of one liter within the pericardial cavity have been reported. Rapid accumulation of as little as 100 mL of fluid following trauma may trigger cardiac tamponade. Other common causes include myocardial rupture, pericarditis, cancer, or even cardiac surgery. Removal of this excess fluid requires insertion of drainage tubes into the pericardial cavity. Premature removal of these drainage tubes, for example, following cardiac surgery, or clot formation within these tubes are causes of this condition. Untreated, cardiac tamponade can lead to death.
Surface Features of the Heart
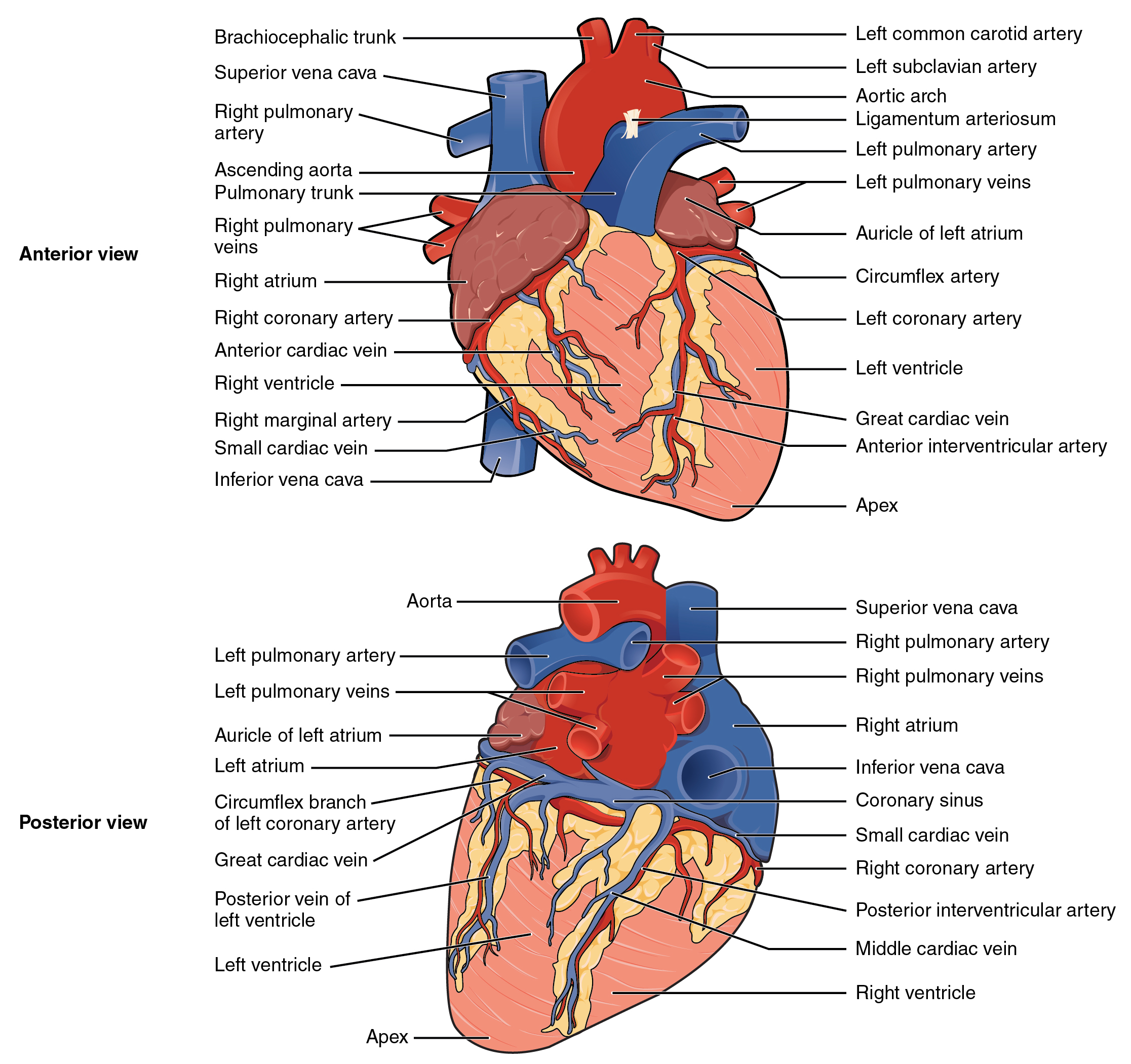
Inside the pericardium, the surface features of the heart are visible, including the four chambers. There is a superficial leaf-like extension of the atria near the superior surface of the heart, one on each side, called an auricle—a name that means “ear like”—because its shape resembles the external ear of a human (Figure). Auricles are relatively thin-walled structures that can fill with blood and empty into the atria or upper chambers of the heart. You may also hear them referred to as atrial appendages. Also prominent is a series of fat-filled grooves, each of which is known as a sulcus (plural = sulci), along the superior surfaces of the heart. Major coronary blood vessels are located in these sulci. The deep coronary sulcus is located between the atria and ventricles. Located between the left and right ventricles are two additional sulci that are not as deep as the coronary sulcus. The anterior interventricular sulcus is visible on the anterior surface of the heart, whereas the posterior interventricular sulcus is visible on the posterior surface of the heart. Figure \(\PageIndex{5}\) illustrates anterior and posterior views of the surface of the heart.
Layers
The wall of the heart is composed of three layers of unequal thickness. From superficial to deep, these are the epicardium, the myocardium, and the endocardium (see Figure \(\PageIndex{4}\)). The outermost layer of the wall of the heart is also the innermost layer of the pericardium, the epicardium, or the visceral pericardium discussed earlier.
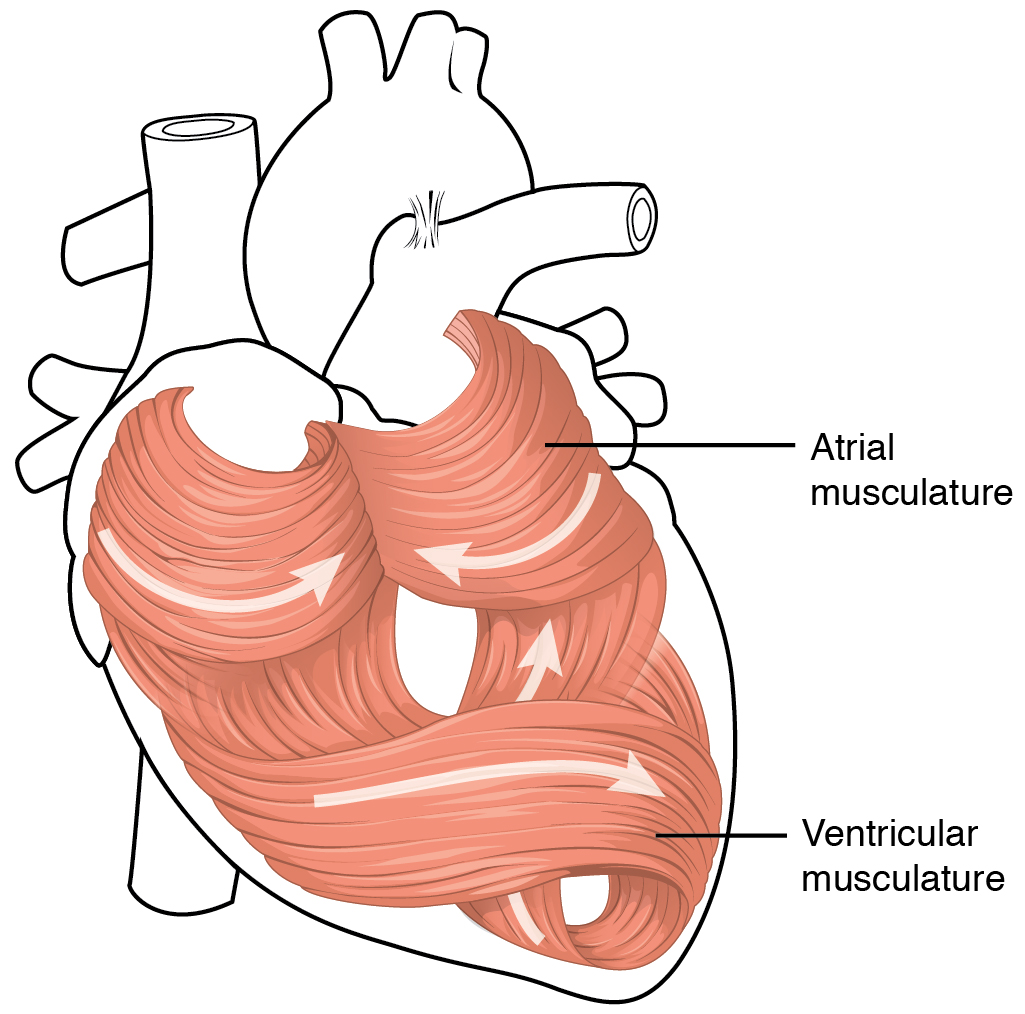
The middle and thickest layer is the myocardium, made largely of cardiac muscle cells. It is built upon a framework of collagenous fibers, plus the blood vessels that supply the myocardium and the nerve fibers that help regulate the heart. It is the contraction of the myocardium that pumps blood through the heart and into the major arteries. The muscle pattern is elegant and complex, as the muscle cells swirl and spiral around the chambers of the heart. They form a figure 8 pattern around the atria and around the bases of the great vessels. Deeper ventricular muscles also form a figure 8 around the two ventricles and proceed toward the apex. More superficial layers of ventricular muscle wrap around both ventricles. This complex swirling pattern allows the heart to pump blood more effectively than a simple linear pattern would. Figure \(\PageIndex{6}\) illustrates the arrangement of muscle cells.
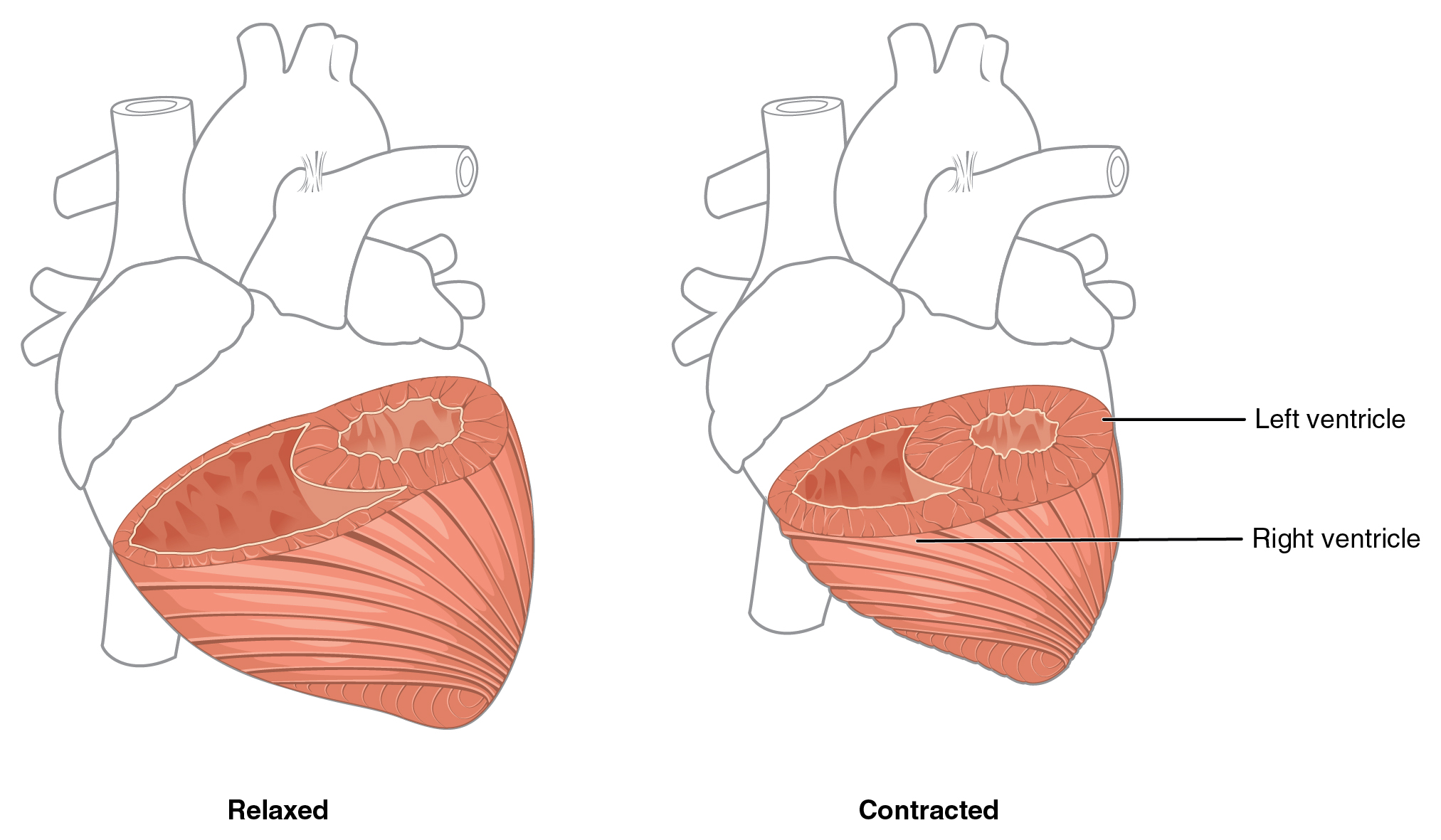
Although the ventricles on the right and left sides pump the same amount of blood per contraction, the muscle of the left ventricle is much thicker and better developed than that of the right ventricle. In order to overcome the high resistance required to pump blood into the long systemic circuit, the left ventricle must generate a great amount of pressure. The right ventricle does not need to generate as much pressure, since the pulmonary circuit is shorter and provides less resistance. Figure \(\PageIndex{7}\) illustrates the differences in muscular thickness needed for each of the ventricles.
The innermost layer of the heart wall, the endocardium, is joined to the myocardium with a thin layer of connective tissue. The endocardium lines the chambers where the blood circulates and covers the heart valves. It is made of simple squamous epithelium called endothelium, which is continuous with the endothelial lining of the blood vessels (Figure \(\PageIndex{4}\)).
Once regarded as a simple lining layer, recent evidence indicates that the endothelium of the endocardium and the coronary capillaries may play active roles in regulating the contraction of the muscle within the myocardium. The endothelium may also regulate the growth patterns of the cardiac muscle cells throughout life, and the endothelins it secretes create an environment in the surrounding tissue fluids that regulates ionic concentrations and states of contractility. Endothelins are potent vasoconstrictors and, in a normal individual, establish a homeostatic balance with other vasoconstrictors and vasodilators.
Internal Structure of the Heart
Recall that the heart’s contraction cycle follows a dual pattern of circulation—the pulmonary and systemic circuits—because of the pairs of chambers that pump blood into the circulation. In order to develop a more precise understanding of cardiac function, it is first necessary to explore the internal anatomical structures in more detail.
Septa of the Heart
The word septum is derived from the Latin for “something that encloses;” in this case, a septum (plural = septa) refers to a wall or partition that divides the heart into chambers. The septa are physical extensions of the myocardium lined with endocardium. Located between the two atria is the interatrial septum. Normally in an adult heart, the interatrial septum bears an oval-shaped depression known as the fossa ovalis, a remnant of an opening in the fetal heart known as the foramen ovale. The foramen ovale allowed blood in the fetal heart to pass directly from the right atrium to the left atrium, allowing some blood to bypass the pulmonary circuit. Within seconds after birth, a flap of tissue known as the septum primum that previously acted as a valve closes the foramen ovale and establishes the typical cardiac circulation pattern.
Between the two ventricles is a second septum known as the interventricular septum. Unlike the interatrial septum, the interventricular septum is normally intact after its formation during fetal development. It is substantially thicker than the interatrial septum, since the ventricles generate far greater pressure when they contract.
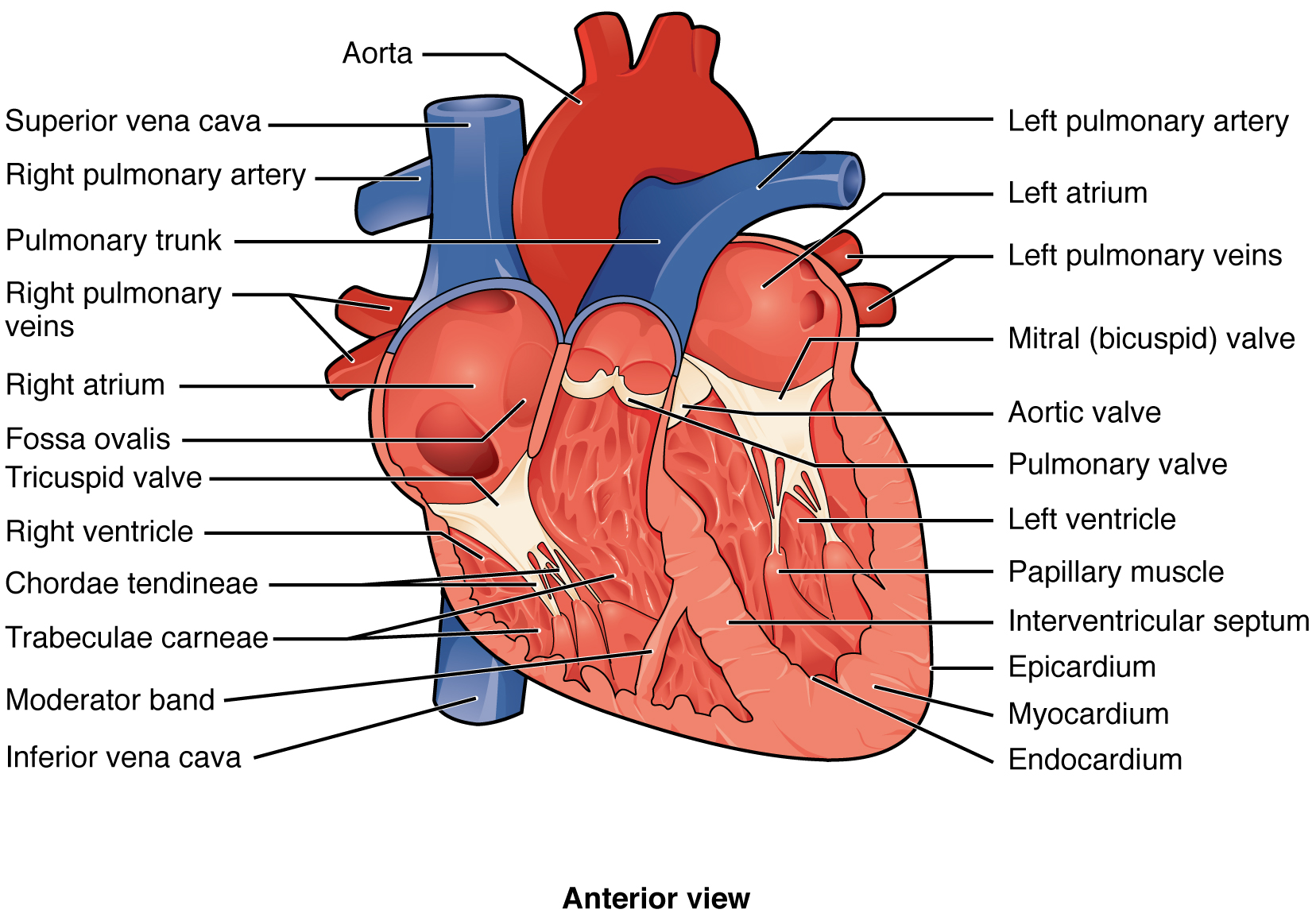
The septum between the atria and ventricles is known as the atrioventricular septum. It is marked by the presence of four openings that allow blood to move from the atria into the ventricles and from the ventricles into the pulmonary trunk and aorta. Located in each of these openings between the atria and ventricles is a valve, a specialized structure that ensures one-way flow of blood. The valves between the atria and ventricles are known generically as atrioventricular valves. The valves at the openings that lead to the pulmonary trunk and aorta are known generically as semilunar valves. The interventricular septum is visible in Figure \(\PageIndex{8}\). In this figure, the atrioventricular septum has been removed to better show the bicupid and tricuspid valves; the interatrial septum is not visible, since its location is covered by the aorta and pulmonary trunk. Since these openings and valves structurally weaken the atrioventricular septum, the remaining tissue is heavily reinforced with dense connective tissue called the cardiac skeleton, or skeleton of the heart. It includes four rings that surround the openings between the atria and ventricles, and the openings to the pulmonary trunk and aorta, and serve as the point of attachment for the heart valves. The cardiac skeleton also provides an important boundary in the heart electrical conduction system.
DISORDERS OF THE ... Heart: Heart Defects
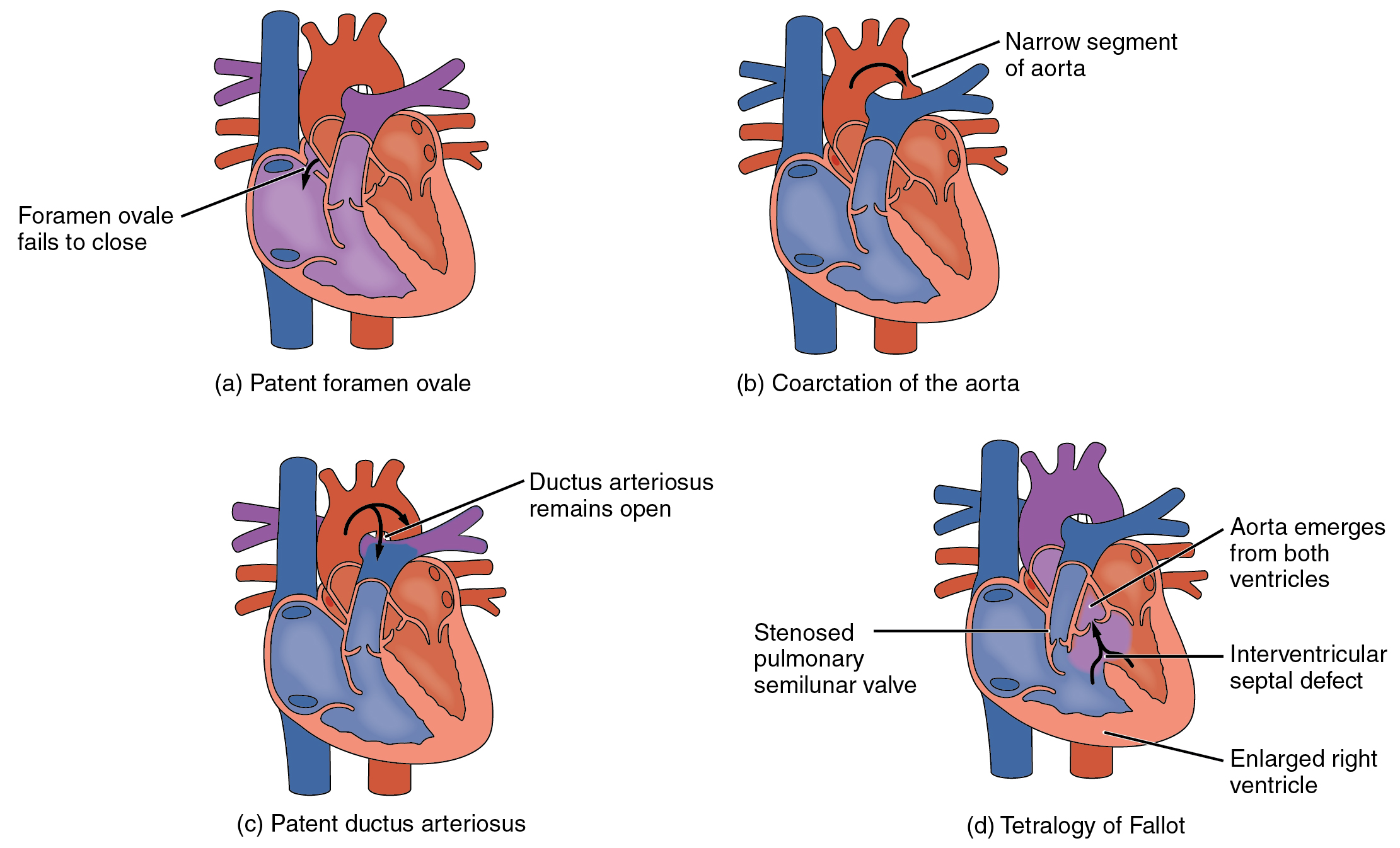
One very common form of interatrial septum pathology is patent foramen ovale, which occurs when the septum primum does not close at birth, and the fossa ovalis is unable to fuse. The word patent is from the Latin root patens for “open.” It may be benign or asymptomatic, perhaps never being diagnosed, or in extreme cases, it may require surgical repair to close the opening permanently. As much as 20–25 percent of the general population may have a patent foramen ovale, but fortunately, most have the benign, asymptomatic version. Patent foramen ovale is normally detected by auscultation of a heart murmur (an abnormal heart sound) and confirmed by imaging with an echocardiogram. Despite its prevalence in the general population, the causes of patent ovale are unknown, and there are no known risk factors. In nonlife-threatening cases, it is better to monitor the condition than to risk heart surgery to repair and seal the opening.
Coarctation of the aorta is a congenital abnormal narrowing of the aorta that is normally located at the insertion of the ligamentum arteriosum, the remnant of the fetal shunt called the ductus arteriosus. If severe, this condition drastically restricts blood flow through the primary systemic artery, which is life threatening. In some individuals, the condition may be fairly benign and not detected until later in life. Detectable symptoms in an infant include difficulty breathing, poor appetite, trouble feeding, or failure to thrive. In older individuals, symptoms include dizziness, fainting, shortness of breath, chest pain, fatigue, headache, and nosebleeds. Treatment involves surgery to resect (remove) the affected region or angioplasty to open the abnormally narrow passageway. Studies have shown that the earlier the surgery is performed, the better the chance of survival.
A patent ductus arteriosus is a congenital condition in which the ductus arteriosus fails to close. The condition may range from severe to benign. Failure of the ductus arteriosus to close results in blood flowing from the higher pressure aorta into the lower pressure pulmonary trunk. This additional fluid moving toward the lungs increases pulmonary pressure and makes respiration difficult. Symptoms include shortness of breath (dyspnea), tachycardia, enlarged heart, a widened pulse pressure, and poor weight gain in infants. Treatments include surgical closure (ligation), manual closure using platinum coils or specialized mesh inserted via the femoral artery or vein, or nonsteroidal anti-inflammatory drugs to block the synthesis of prostaglandin E2, which maintains the vessel in an open position. If untreated, the condition can result in congestive heart failure.
Septal defects are not uncommon in individuals and may be congenital or caused by various disease processes. Tetralogy of Fallot is a congenital condition that may also occur from exposure to unknown environmental factors; it occurs when there is an opening in the interventricular septum caused by blockage of the pulmonary trunk, normally at the pulmonary semilunar valve. This allows blood that is relatively low in oxygen from the right ventricle to flow into the left ventricle and mix with the blood that is relatively high in oxygen. Symptoms include a distinct heart murmur, low blood oxygen percent saturation, dyspnea or difficulty in breathing, polycythemia, broadening (clubbing) of the fingers and toes, and in children, difficulty in feeding or failure to grow and develop. It is the most common cause of cyanosis following birth. The term “tetralogy” is derived from the four components of the condition, although only three may be present in an individual patient: pulmonary infundibular stenosis (rigidity of the pulmonary valve), overriding aorta (the aorta is shifted above both ventricles), ventricular septal defect (opening), and right ventricular hypertrophy (enlargement of the right ventricle). Other heart defects may also accompany this condition, which is typically confirmed by echocardiography imaging. Tetralogy of Fallot occurs in approximately 400 out of one million live births. Normal treatment involves extensive surgical repair, including the use of stents to redirect blood flow and replacement of valves and patches to repair the septal defect, but the condition has a relatively high mortality. Survival rates are currently 75 percent during the first year of life; 60 percent by 4 years of age; 30 percent by 10 years; and 5 percent by 40 years.
In the case of severe septal defects, including both tetralogy of Fallot and patent foramen ovale, failure of the heart to develop properly can lead to a condition commonly known as a “blue baby.” Regardless of normal skin pigmentation, individuals with this condition have an insufficient supply of oxygenated blood, which leads to cyanosis, a blue or purple coloration of the skin, especially when active.
Septal defects are commonly first detected through auscultation, listening to the chest using a stethoscope. In this case, instead of hearing normal heart sounds attributed to the flow of blood and closing of heart valves, unusual heart sounds may be detected. This is often followed by medical imaging to confirm or rule out a diagnosis. In many cases, treatment may not be needed. Some common congenital heart defects are illustrated in Figure \(\PageIndex{9}\).
Right Atrium
The right atrium serves as the receiving chamber for blood returning to the heart from the systemic circulation. The two major systemic veins, the superior and inferior venae cavae, and the large coronary vein called the coronary sinus that drains the heart myocardium empty into the right atrium. The superior vena cava drains blood from regions superior to the diaphragm: the head, neck, upper limbs, and the thoracic region. It empties into the superior and posterior portions of the right atrium. The inferior vena cava drains blood from areas inferior to the diaphragm: the lower limbs and abdominopelvic region of the body. It, too, empties into the posterior portion of the atria, but inferior to the opening of the superior vena cava. Immediately superior and slightly medial to the opening of the inferior vena cava on the posterior surface of the atrium is the opening of the coronary sinus. This thin-walled vessel drains most of the coronary veins that return systemic blood from the heart. The majority of the internal heart structures discussed in this and subsequent sections are illustrated in Figure \(\PageIndex{8}\).
While the bulk of the internal surface of the right atrium is smooth, the depression of the fossa ovalis is medial, and the anterior surface demonstrates prominent ridges of muscle called the pectinate muscles. The right auricle also has pectinate muscles. The left atrium does not have pectinate muscles except in the auricle.
The atria receive venous blood on a nearly continuous basis, preventing venous flow from stopping while the ventricles are contracting. While most ventricular filling occurs while the atria are relaxed, they do demonstrate a contractile phase and actively pump blood into the ventricles just prior to ventricular contraction. The opening between the atrium and ventricle is guarded by the tricuspid valve.
Right Ventricle
The right ventricle receives blood from the right atrium through the tricuspid valve. Each flap of the valve is attached to strong strands of connective tissue, the chordae tendineae, literally “tendinous cords,” or sometimes more poetically referred to as “heart strings.” There are several chordae tendineae associated with each of the flaps. They are composed of approximately 80 percent collagenous fibers with the remainder consisting of elastic fibers and endothelium. They connect each of the flaps to a papillary muscle that extends from the inferior ventricular surface. There are three papillary muscles in the right ventricle, called the anterior, posterior, and septal muscles, which correspond to the three sections of the valves.
When the myocardium of the ventricle contracts, pressure within the ventricular chamber rises. Blood, like any fluid, flows from higher pressure to lower pressure areas, in this case, toward the pulmonary trunk and the atrium. To prevent any potential backflow, the papillary muscles also contract, generating tension on the chordae tendineae. This prevents the flaps of the valves from being forced into the atria and regurgitation of the blood back into the atria during ventricular contraction. Figure \(\PageIndex{10}\) shows papillary muscles and chordae tendineae attached to the tricuspid valve.
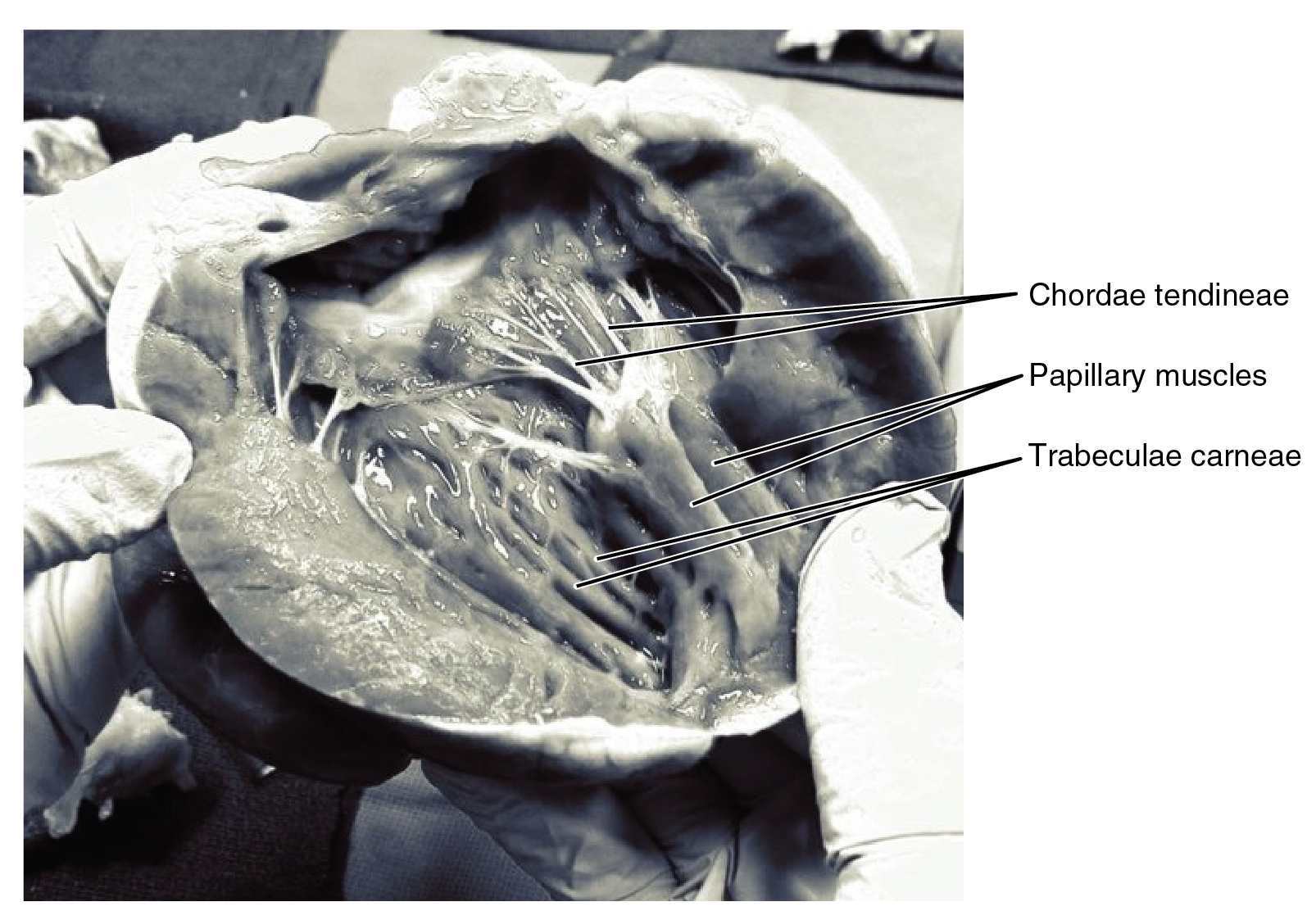
The walls of the ventricle are lined with trabeculae carneae, ridges of cardiac muscle covered by endocardium. In addition to these muscular ridges, a band of cardiac muscle, also covered by endocardium, known as the moderator band (see Figure \(\PageIndex{8}\)) reinforces the thin walls of the right ventricle and plays a crucial role in cardiac conduction. It arises from the inferior portion of the interventricular septum and crosses the interior space of the right ventricle to connect with the inferior papillary muscle.
When the right ventricle contracts, it ejects blood into the pulmonary trunk, which branches into the left and right pulmonary arteries that carry it to each lung. The superior surface of the right ventricle begins to taper as it approaches the pulmonary trunk. At the base of the pulmonary trunk is the pulmonary semilunar valve that prevents backflow from the pulmonary trunk.
Left Atrium
After exchange of gases in the pulmonary capillaries, blood returns to the left atrium high in oxygen via one of the four pulmonary veins. While the left atrium does not contain pectinate muscles, it does have an auricle that includes these pectinate ridges. Blood flows nearly continuously from the pulmonary veins back into the atrium, which acts as the receiving chamber, and from here through an opening into the left ventricle. Most blood flows passively into the heart while both the atria and ventricles are relaxed, but toward the end of the ventricular relaxation period, the left atrium will contract, pumping blood into the ventricle. This atrial contraction accounts for approximately 20 percent of ventricular filling. The opening between the left atrium and ventricle is guarded by the mitral valve.
Left Ventricle
Recall that, although both sides of the heart will pump the same amount of blood, the muscular layer is much thicker in the left ventricle compared to the right (see Figure \(\PageIndex{7}\)). Like the right ventricle, the left also has trabeculae carneae, but there is no moderator band. The mitral valve is connected to papillary muscles via chordae tendineae. There are two papillary muscles on the left—the anterior and posterior—as opposed to three on the right.
The left ventricle is the major pumping chamber for the systemic circuit; it ejects blood into the aorta through the aortic semilunar valve.
Heart Valve Structure and Function
A transverse section through the heart slightly above the level of the atrioventricular septum reveals all four heart valves along the same plane (Figure \(\PageIndex{11}\)). The valves ensure unidirectional blood flow through the heart. Between the right atrium and the right ventricle is the right atrioventricular valve, or tricuspid valve. It typically consists of three flaps, or leaflets, made of endocardium reinforced with additional connective tissue. The flaps are connected by chordae tendineae to the papillary muscles, which control the opening and closing of the valves.
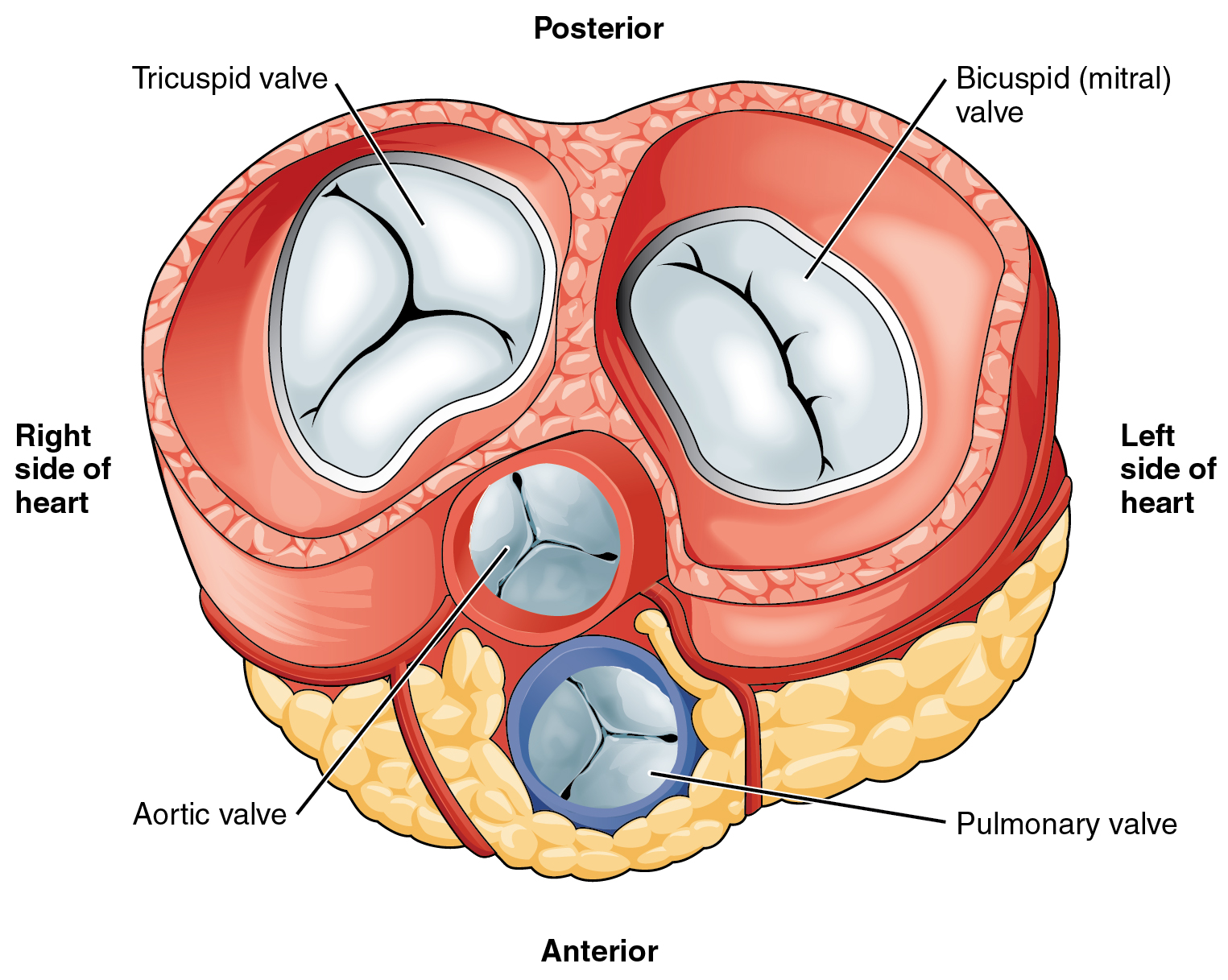
Emerging from the right ventricle at the base of the pulmonary trunk is the pulmonary semilunar valve, or the pulmonary valve; it is also known as the pulmonic valve or the right semilunar valve. The pulmonary valve is comprised of three small flaps of endothelium reinforced with connective tissue. When the ventricle relaxes, the pressure differential causes blood to flow back into the ventricle from the pulmonary trunk. This flow of blood fills the pocket-like flaps of the pulmonary valve, causing the valve to close and producing an audible sound. Unlike the atrioventricular valves, there are no papillary muscles or chordae tendineae associated with the pulmonary valve.
Located at the opening between the left atrium and left ventricle is the mitral valve, also called the bicuspid valve or the left atrioventricular valve. Structurally, this valve consists of two cusps, known as the anterior medial cusp and the posterior medial cusp, compared to the three cusps of the tricuspid valve. In a clinical setting, the valve is referred to as the mitral valve, rather than the bicuspid valve. The two cusps of the mitral valve are attached by chordae tendineae to two papillary muscles that project from the wall of the ventricle.
At the base of the aorta is the aortic semilunar valve, or the aortic valve, which prevents backflow from the aorta. It normally is composed of three flaps. When the ventricle relaxes and blood attempts to flow back into the ventricle from the aorta, blood will fill the cusps of the valve, causing it to close and producing an audible sound.
In Figure19.1.12.a, the two atrioventricular valves are open and the two semilunar valves are closed. This occurs when both atria and ventricles are relaxed and when the atria contract to pump blood into the ventricles. Figure19.1.12.b shows a frontal view. Although only the left side of the heart is illustrated, the process is virtually identical on the right.
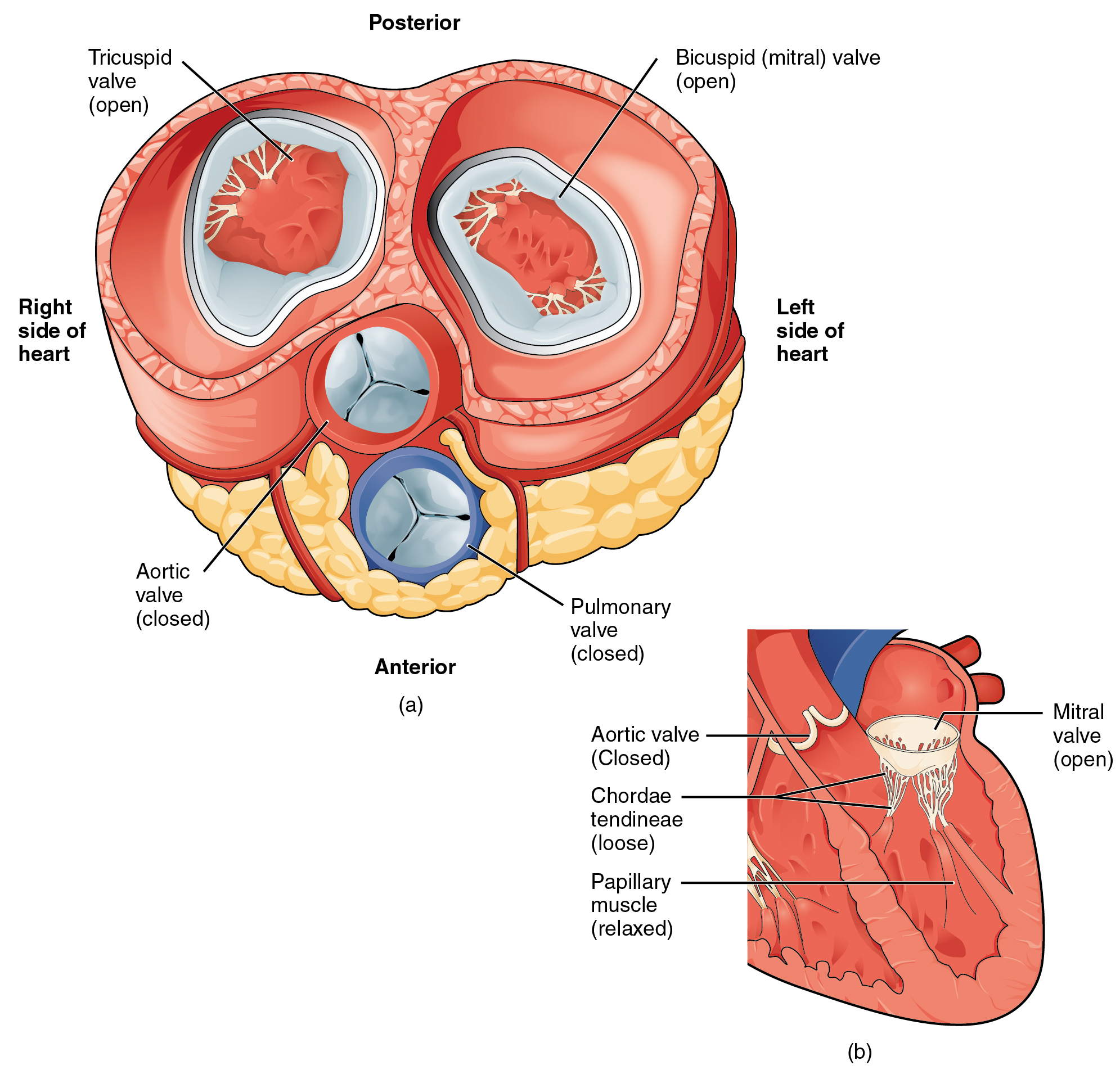
Figure \(\PageIndex{13}\).a shows the atrioventricular valves closed while the two semilunar valves are open. This occurs when the ventricles contract to eject blood into the pulmonary trunk and aorta. Closure of the two atrioventricular valves prevents blood from being forced back into the atria. This stage can be seen from a frontal view in Figure19.1.13.b.
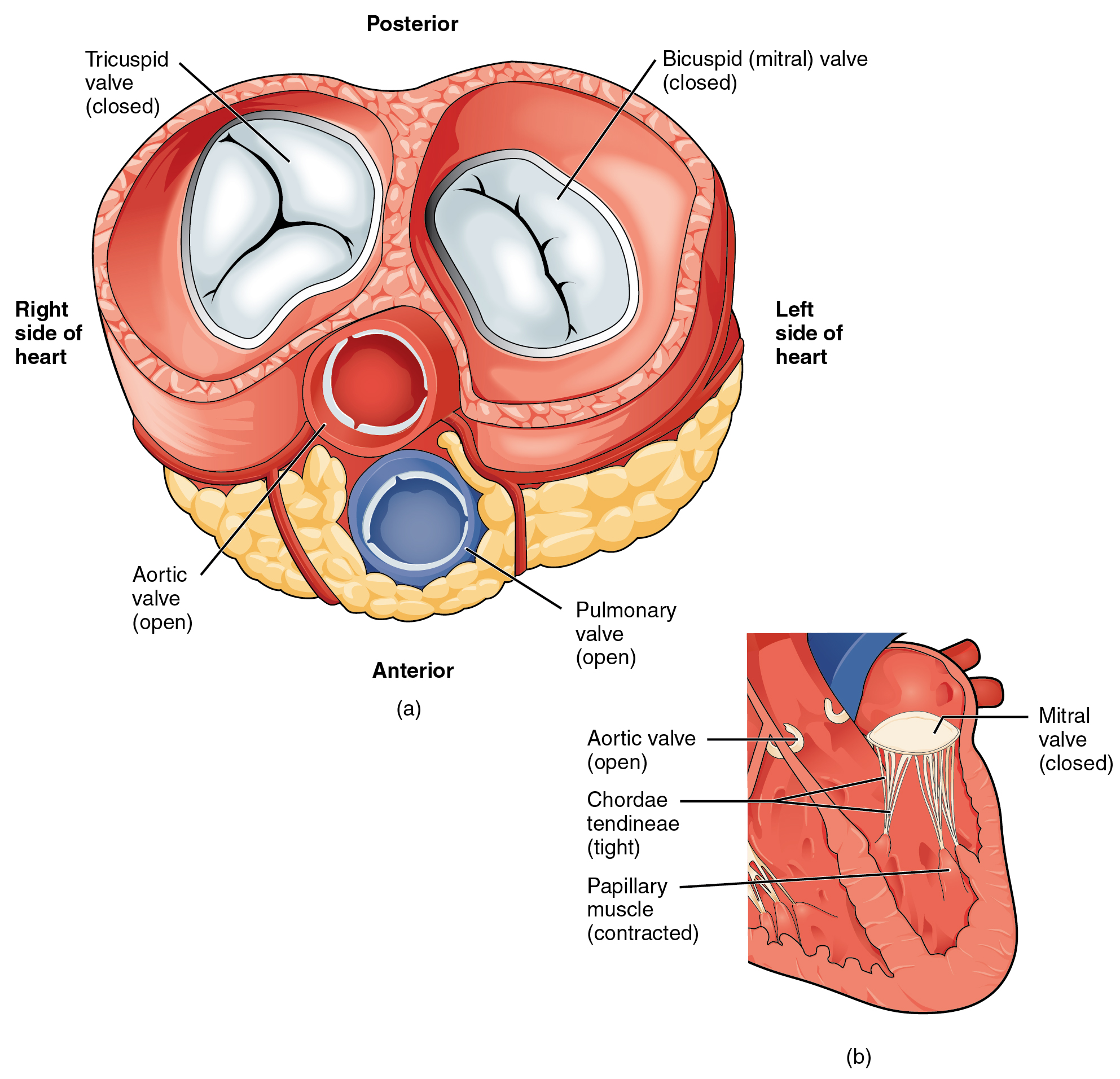
When the ventricles begin to contract, pressure within the ventricles rises and blood flows toward the area of lowest pressure, which is initially in the atria. This backflow causes the cusps of the tricuspid and mitral (bicuspid) valves to close. These valves are tied down to the papillary muscles by chordae tendineae. During the relaxation phase of the cardiac cycle, the papillary muscles are also relaxed and the tension on the chordae tendineae is slight (see Figure \(\PageIndex{12}\).b). However, as the myocardium of the ventricle contracts, so do the papillary muscles. This creates tension on the chordae tendineae (see Figure19.1.13.b), helping to hold the cusps of the atrioventricular valves in place and preventing them from being blown back into the atria.
The aortic and pulmonary semilunar valves lack the chordae tendineae and papillary muscles associated with the atrioventricular valves. Instead, they consist of pocket-like folds of endocardium reinforced with additional connective tissue. When the ventricles relax and the change in pressure forces the blood toward the ventricles, the blood presses against these cusps and seals the openings.

قم بزيارة هذا الموقع لمراقبة مخطط صدى القلب لفتح وإغلاق صمامات القلب الفعلية. على الرغم من أن جزءًا كبيرًا من القلب قد تم «إزالته» من حلقة GIF هذه بحيث لا تكون الأوتار الحبلية مرئية، فما سبب أهمية وجودها للصمامات الأذينية البطينية (ثلاثية الشرفات والمترالية) أكثر من الصمامات نصف القمرية (الأبهرية والرئوية)؟
اضطرابات... صمامات القلب
عندما لا تعمل صمامات القلب بشكل صحيح، غالبًا ما توصف بأنها غير فعالة وتؤدي إلى أمراض صمامات القلب، والتي يمكن أن تتراوح من حميدة إلى قاتلة. بعض هذه الحالات خلقية، أي أن الفرد ولد بعيب، بينما قد يُعزى البعض الآخر إلى عمليات المرض أو الصدمة. يتم علاج بعض الأعطال بالأدوية، والبعض الآخر يحتاج إلى جراحة، والبعض الآخر قد يكون خفيفًا بدرجة كافية بحيث تتم مراقبة الحالة فقط لأن العلاج قد يؤدي إلى عواقب أكثر خطورة.
غالبًا ما تحدث الاضطرابات الصمامية بسبب التهاب القلب أو التهاب القلب. أحد الأسباب الشائعة لهذا الالتهاب هو الحمى الروماتيزمية، أو الحمى القرمزية، وهي استجابة مناعية ذاتية لوجود بكتيريا، المكورات العقدية المقيحة، وعادة ما تكون مرضًا في مرحلة الطفولة.
في حين أن أيًا من صمامات القلب قد يكون متورطًا في اضطرابات الصمام، فإن القلس التاجي هو الأكثر شيوعًا، حيث يتم اكتشافه في حوالي 2 بالمائة من السكان، والصمام شبه القمري الرئوي هو الأقل تعرضًا للإصابة. عندما يتعطل الصمام، غالبًا ما يتعطل تدفق الدم إلى المنطقة. سيتم وصف التدفق غير الكافي للدم الناتج إلى هذه المنطقة بشكل عام بأنه عدم كفاية. يُطلق على النوع المحدد من القصور اسم الصمام المعني: قصور الشريان الأورطي، القصور التاجي، القصور ثلاثي الشرفات، أو القصور الرئوي.
إذا أُجبرت إحدى شرفات الصمام على التراجع بفعل قوة الدم، يُشار إلى الحالة باسم الصمام المتدلي. قد يحدث التدلي في حالة تلف الحبل الوتري أو كسره، مما يؤدي إلى فشل آلية الإغلاق. يؤدي فشل الصمام في الإغلاق بشكل صحيح إلى تعطيل التدفق الطبيعي للدم في اتجاه واحد ويؤدي إلى الارتجاع، عندما يتدفق الدم للخلف عن مساره الطبيعي. باستخدام سماعة الطبيب، ينتج عن اضطراب التدفق الطبيعي للدم نفخة قلبية.
التضيق هو حالة تصبح فيها صمامات القلب صلبة وقد تتكلس بمرور الوقت. يتداخل فقدان مرونة الصمام مع الوظيفة الطبيعية وقد يتسبب في عمل القلب بجهد أكبر لدفع الدم عبر الصمام، مما يؤدي في النهاية إلى إضعاف القلب. يؤثر تضيق الأبهر على حوالي 2 بالمائة من السكان الذين تزيد أعمارهم عن 65 عامًا، وترتفع النسبة إلى حوالي 4 بالمائة لدى الأفراد الذين تزيد أعمارهم عن 85 عامًا. من حين لآخر، يتمزق واحد أو أكثر من الأوتار الحبلية أو قد تموت العضلة الحليمية نفسها كعنصر من عناصر احتشاء عضلة القلب (نوبة قلبية). في هذه الحالة، ستتدهور حالة المريض بشكل كبير وسريع، وقد يتطلب الأمر التدخل الجراحي الفوري.
يعد التسمع، أو الاستماع إلى أصوات قلب المريض، أحد أكثر أدوات التشخيص فائدة، لأنه مثبت وآمن وغير مكلف. مصطلح التسمع مشتق من الكلمة اللاتينية التي تعني «الاستماع»، وقد تم استخدام هذه التقنية لأغراض التشخيص منذ عهد المصريين القدماء. ستؤدي اضطرابات الصمام والحاجز إلى أصوات قلب غير طبيعية. في حالة اكتشاف اضطراب صمامي أو الاشتباه به، قد يُطلب إجراء اختبار يسمى مخطط صدى القلب، أو ببساطة «الصدى». تخطيط صدى القلب عبارة عن تصوير بالموجات فوق الصوتية للقلب ويمكن أن يساعد في تشخيص اضطرابات الصمامات بالإضافة إلى مجموعة متنوعة من أمراض القلب.

قم بزيارة هذا الموقع للتنزيل المجاني، بما في ذلك الرسوم المتحركة الممتازة وصوت أصوات القلب.
الاتصال الوظيفي
طبيب القلب
أطباء القلب هم أطباء متخصصون في تشخيص وعلاج أمراض القلب. بعد الانتهاء من 4 سنوات في كلية الطب، يكمل أطباء القلب الإقامة لمدة ثلاث سنوات في الطب الباطني تليها ثلاث سنوات إضافية أو أكثر في أمراض القلب. بعد هذه الفترة التي تبلغ 10 سنوات من التدريب الطبي والخبرة السريرية، يتأهلون لفحص صارم لمدة يومين يديره مجلس الطب الباطني الذي يختبر تدريبهم الأكاديمي وقدراتهم السريرية، بما في ذلك التشخيص والعلاج. بعد الانتهاء بنجاح من هذا الفحص، يصبح الطبيب طبيب قلب معتمد من مجلس الإدارة. قد تتم دعوة بعض أطباء القلب الحاصلين على شهادة البورد الأمريكي ليصبحوا زملاء في الكلية الأمريكية لأمراض القلب (FACC). يتم منح هذا التقدير المهني للأطباء المتميزين على أساس الجدارة، بما في ذلك أوراق الاعتماد والإنجازات والمساهمات المجتمعية في طب القلب والأوعية الدموية.

قم بزيارة هذا الموقع لمعرفة المزيد عن أطباء القلب.
الاتصال الوظيفي
تقني/فني القلب والأوعية الدموية
تقنيو/فنيو القلب والأوعية الدموية هم من المهنيين المدربين الذين يقومون بمجموعة متنوعة من تقنيات التصوير، مثل التصوير بالموجات فوق الصوتية أو تخطيط صدى القلب، التي يستخدمها الأطباء لتشخيص وعلاج أمراض القلب. تتطلب جميع هذه الوظائف تقريبًا درجة الزمالة، ويحصل هؤلاء الفنيون على راتب متوسط قدره 49,410 دولارًا اعتبارًا من مايو 2010، وفقًا لمكتب إحصاءات العمل الأمريكي. والنمو داخل هذا المجال سريع، ومن المتوقع أن يصل إلى 29 في المائة من عام 2010 إلى عام 2020.
هناك تداخل كبير ومهارات تكميلية بين فنيي القلب وفنيي الأوعية الدموية، وبالتالي غالبًا ما يستخدم مصطلح فني القلب والأوعية الدموية. تتطلب الشهادات الخاصة داخل المجال توثيق الخبرة المناسبة وإكمال اختبارات الشهادات الإضافية والمكلفة في كثير من الأحيان. تشمل هذه التخصصات الفرعية فني تحليل الإيقاع المعتمد (CRAT)، وفني تخطيط القلب المعتمد (CCT)، وأخصائي الموجات فوق الصوتية للقلب الخلقية المسجل (RCCS)، وأخصائي الفيزيولوجيا الكهربية للقلب المسجل (RCES)، وأخصائي التدخل الجراحي للقلب والأوعية الدموية المسجل (RCIS)، وأخصائي الموجات فوق الصوتية للقلب المسجل (RCS)، أخصائي الأوعية الدموية المسجل (RVS) وأخصائي الموجات فوق الصوتية المسجل في علم الأوردة (RPHS).

قم بزيارة هذا الموقع لمزيد من المعلومات حول تقنيين/فنيي القلب والأوعية الدموية.
الدورة الدموية التاجية
سوف تتذكر أن القلب عبارة عن مضخة رائعة تتكون بشكل كبير من خلايا عضلة القلب التي تنشط بشكل لا يصدق طوال الحياة. مثل جميع الخلايا الأخرى، تتطلب خلية عضلة القلب إمدادًا موثوقًا بالأكسجين والمواد المغذية، وطريقة لإزالة النفايات، لذلك فهي تحتاج إلى دورة دموية التاجية مخصصة ومعقدة وواسعة النطاق. وبسبب نشاط القلب الحرج والذي لا يتوقف تقريبًا طوال الحياة، فإن هذه الحاجة إلى إمدادات الدم أكبر من تلك الخاصة بالخلية العادية. ومع ذلك، فإن الدورة الدموية التاجية ليست مستمرة؛ بل إنها تدور لتصل إلى ذروتها عندما تكون عضلة القلب مسترخية وتتوقف تقريبًا أثناء انقباضها.
الشرايين التاجية
توفر الشرايين التاجية الدم لعضلة القلب ومكونات القلب الأخرى. يؤدي الجزء الأول من الشريان الأورطي بعد ظهوره من البطين الأيسر إلى ظهور الشرايين التاجية. هناك ثلاثة توسعات في جدار الشريان الأورطي أعلى بقليل من الصمام الأبهري شبه القمري. يؤدي اثنان منها، وهما الجيب الأبهري الخلفي الأيسر والجيب الأبهري الأمامي، إلى ظهور الشرايين التاجية اليمنى واليسرى على التوالي. عادةً لا يؤدي الجيب الثالث، وهو الجيب الأبهري الخلفي الأيمن، إلى تكوين وعاء. تُسمى فروع الأوعية التاجية التي تبقى على سطح الشريان وتتبع التسيل بالشرايين التاجية اللبيفية.
يقوم الشريان التاجي الأيسر بتوزيع الدم على الجانب الأيسر من القلب والأذين الأيسر والبطين والحاجز بين البطينين. ينشأ الشريان المحيطي من الشريان التاجي الأيسر ويتبع التلم التاجي إلى اليسار. في النهاية، سوف يندمج مع الفروع الصغيرة للشريان التاجي الأيمن. الشريان الأمامي بين البطينين الأكبر، والمعروف أيضًا باسم الشريان الأمامي النازل الأيسر (LAD)، هو الفرع الرئيسي الثاني الناشئ عن الشريان التاجي الأيسر. يتبع التلم الأمامي بين البطينين حول الجذع الرئوي. على طول الطريق، يؤدي ذلك إلى ظهور العديد من الفروع الصغيرة التي تتصل بفروع الشريان الخلفي بين البطينين، وتشكل مفاغرة. المفاغرة هي منطقة تتحد فيها الأوعية لتكوين روابط تسمح عادةً للدم بالانتقال إلى المنطقة حتى لو كان هناك انسداد جزئي في فرع آخر. المفاغرة في القلب صغيرة جدًا. لذلك، تكون هذه القدرة مقيدة إلى حد ما في القلب، لذلك غالبًا ما يؤدي انسداد الشريان التاجي إلى موت الخلايا (احتشاء عضلة القلب) التي يوفرها الوعاء المعين.
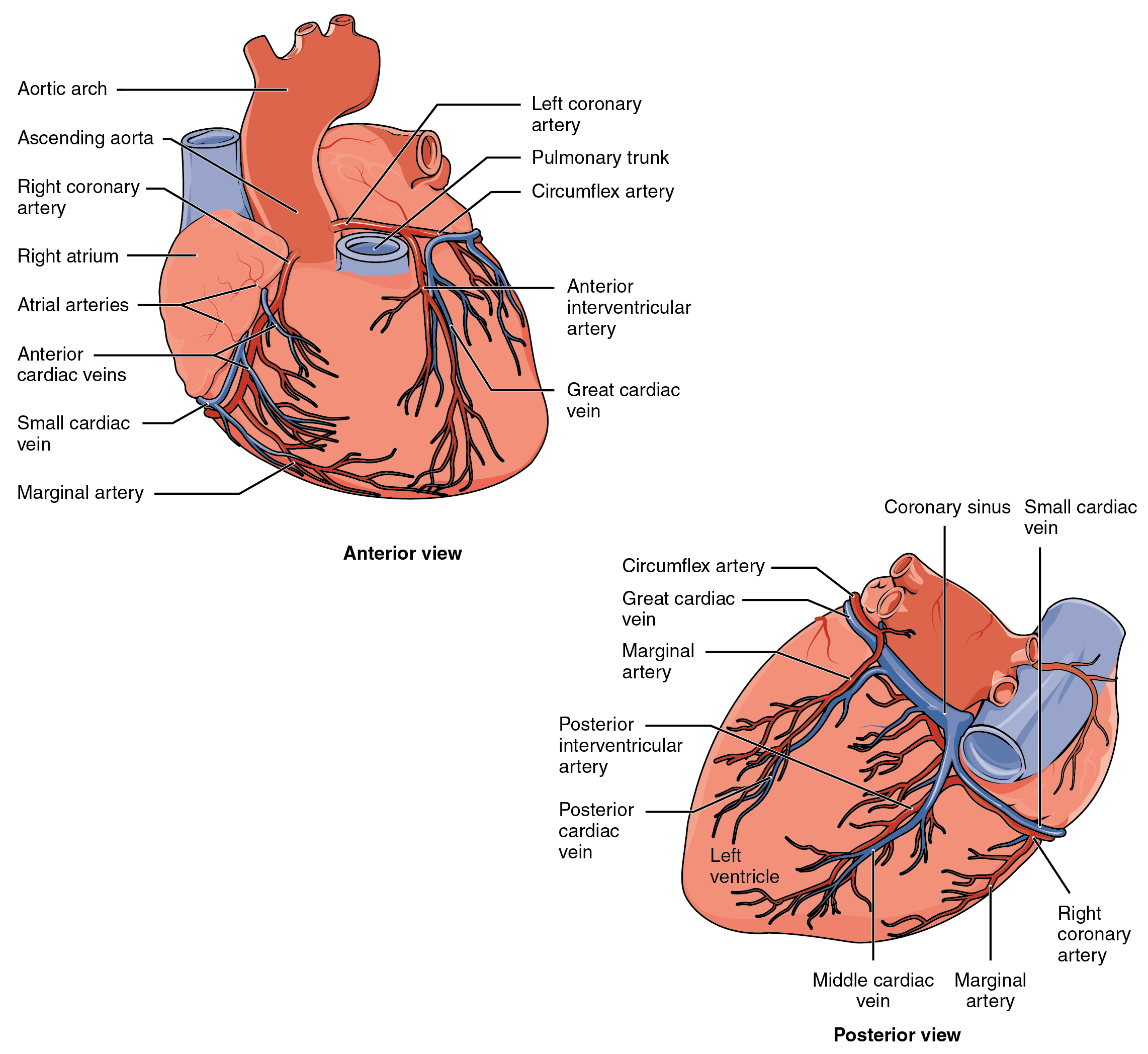
يمتد الشريان التاجي الأيمن على طول التلم التاجي ويوزع الدم إلى الأذين الأيمن وأجزاء من كلا البطينين ونظام التوصيل القلبي. عادةً ما ينشأ واحد أو أكثر من الشرايين الهامشية من الشريان التاجي الأيمن السفلي للأذين الأيمن. تقوم الشرايين الهامشية بتزويد الدم إلى الأجزاء السطحية من البطين الأيمن. على السطح الخلفي للقلب، يؤدي الشريان التاجي الأيمن إلى ظهور الشريان الخلفي بين البطينين، المعروف أيضًا باسم الشريان الخلفي الهابط. يمتد على طول الجزء الخلفي من التلم بين البطينين باتجاه قمة القلب، مما يؤدي إلى ظهور فروع تغذي الحاجز بين البطينين وأجزاء من كلا البطينين. الشكل\(\PageIndex{14}\) presents views of the coronary circulation from both the anterior and posterior views.
DISEASES OF THE ... Heart: Myocardial Infarction
Myocardial infarction (MI) is the formal term for what is commonly referred to as a heart attack. It normally results from a lack of blood flow (ischemia) and oxygen (hypoxia) to a region of the heart, resulting in death of the cardiac muscle cells. An MI often occurs when a coronary artery is blocked by the buildup of atherosclerotic plaque consisting of lipids, cholesterol and fatty acids, and white blood cells, primarily macrophages. It can also occur when a portion of an unstable atherosclerotic plaque travels through the coronary arterial system and lodges in one of the smaller vessels. The resulting blockage restricts the flow of blood and oxygen to the myocardium and causes death of the tissue. MIs may be triggered by excessive exercise, in which the partially occluded artery is no longer able to pump sufficient quantities of blood, or severe stress, which may induce spasm of the smooth muscle in the walls of the vessel.
In the case of acute MI, there is often sudden pain beneath the sternum (retrosternal pain) called angina pectoris, often radiating down the left arm in males but not in female patients. Until this anomaly between the sexes was discovered, many female patients suffering MIs were misdiagnosed and sent home. In addition, patients typically present with difficulty breathing and shortness of breath (dyspnea), irregular heartbeat (palpations), nausea and vomiting, sweating (diaphoresis), anxiety, and fainting (syncope), although not all of these symptoms may be present. Many of the symptoms are shared with other medical conditions, including anxiety attacks and simple indigestion, so differential diagnosis is critical. It is estimated that between 22 and 64 percent of MIs present without any symptoms.
An MI can be confirmed by examining the patient’s ECG, which frequently reveals alterations in the ST and Q components. Some classification schemes of MI are referred to as ST-elevated MI (STEMI) and non-elevated MI (non-STEMI). In addition, echocardiography or cardiac magnetic resonance imaging may be employed. Common blood tests indicating an MI include elevated levels of creatine kinase MB (an enzyme that catalyzes the conversion of creatine to phosphocreatine, consuming ATP) and cardiac troponin (the regulatory protein for muscle contraction), both of which are released by damaged cardiac muscle cells.
Immediate treatments for MI are essential and include administering supplemental oxygen, aspirin that helps to break up clots, and nitroglycerine administered sublingually (under the tongue) to facilitate its absorption. Despite its unquestioned success in treatments and use since the 1880s, the mechanism of nitroglycerine is still incompletely understood but is believed to involve the release of nitric oxide, a known vasodilator, and endothelium-derived releasing factor, which also relaxes the smooth muscle in the tunica media of coronary vessels. Longer-term treatments include injections of thrombolytic agents such as streptokinase that dissolve the clot, the anticoagulant heparin, balloon angioplasty and stents to open blocked vessels, and bypass surgery to allow blood to pass around the site of blockage. If the damage is extensive, coronary replacement with a donor heart or coronary assist device, a sophisticated mechanical device that supplements the pumping activity of the heart, may be employed. Despite the attention, development of artificial hearts to augment the severely limited supply of heart donors has proven less than satisfactory but will likely improve in the future.
MIs may trigger cardiac arrest, but the two are not synonymous. Important risk factors for MI include cardiovascular disease, age, smoking, high blood levels of the low-density lipoprotein (LDL, often referred to as “bad” cholesterol), low levels of high-density lipoprotein (HDL, or “good” cholesterol), hypertension, diabetes mellitus, obesity, lack of physical exercise, chronic kidney disease, excessive alcohol consumption, and use of illegal drugs.
Coronary Veins
Coronary veins drain the heart and generally parallel the large surface arteries (see Figure \(\PageIndex{14}\)). The great cardiac vein can be seen initially on the surface of the heart following the interventricular sulcus, but it eventually flows along the coronary sulcus into the coronary sinus on the posterior surface. The great cardiac vein initially parallels the anterior interventricular artery and drains the areas supplied by this vessel. It receives several major branches, including the posterior cardiac vein, the middle cardiac vein, and the small cardiac vein. The posterior cardiac vein parallels and drains the areas supplied by the marginal artery branch of the circumflex artery. The middle cardiac vein parallels and drains the areas supplied by the posterior interventricular artery. The small cardiac vein parallels the right coronary artery and drains the blood from the posterior surfaces of the right atrium and ventricle. The coronary sinus is a large, thin-walled vein on the posterior surface of the heart lying within the atrioventricular sulcus and emptying directly into the right atrium. The anterior cardiac veins parallel the small cardiac arteries and drain the anterior surface of the right ventricle. Unlike these other cardiac veins, it bypasses the coronary sinus and drains directly into the right atrium.
DISEASES OF THE ... Heart: Coronary Artery Disease
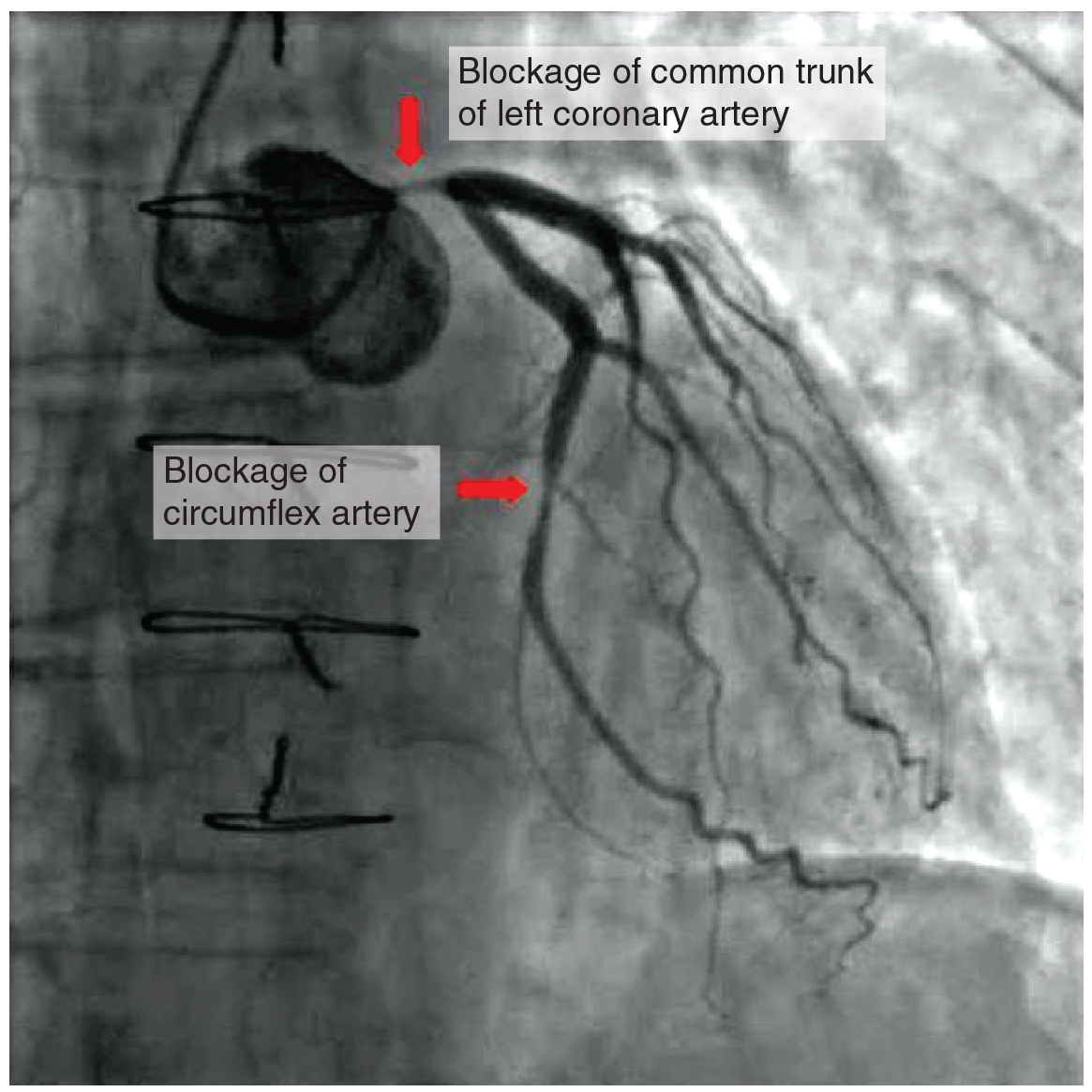
Coronary artery disease is the leading cause of death worldwide. It occurs when the buildup of plaque—a fatty material including cholesterol, connective tissue, white blood cells, and some smooth muscle cells—within the walls of the arteries obstructs the flow of blood and decreases the flexibility or compliance of the vessels. This condition is called atherosclerosis, a hardening of the arteries that involves the accumulation of plaque. As the coronary blood vessels become occluded, the flow of blood to the tissues will be restricted, a condition called ischemia that causes the cells to receive insufficient amounts of oxygen, called hypoxia. Figure \(\PageIndex{15}\) shows the blockage of coronary arteries highlighted by the injection of dye. Some individuals with coronary artery disease report pain radiating from the chest called angina pectoris, but others remain asymptomatic. If untreated, coronary artery disease can lead to MI or a heart attack.
The disease progresses slowly and often begins in children and can be seen as fatty “streaks” in the vessels. It then gradually progresses throughout life. Well-documented risk factors include smoking, family history, hypertension, obesity, diabetes, high alcohol consumption, lack of exercise, stress, and hyperlipidemia or high circulating levels of lipids in the blood. Treatments may include medication, changes to diet and exercise, angioplasty with a balloon catheter, insertion of a stent, or coronary bypass procedure.
Angioplasty is a procedure in which the occlusion is mechanically widened with a balloon. A specialized catheter with an expandable tip is inserted into a superficial vessel, normally in the leg, and then directed to the site of the occlusion. At this point, the balloon is inflated to compress the plaque material and to open the vessel to increase blood flow. Then, the balloon is deflated and retracted. A stent consisting of a specialized mesh is typically inserted at the site of occlusion to reinforce the weakened and damaged walls. Stent insertions have been routine in cardiology for more than 40 years.
Coronary bypass surgery may also be performed. This surgical procedure grafts a replacement vessel obtained from another, less vital portion of the body to bypass the occluded area. This procedure is clearly effective in treating patients experiencing a MI, but overall does not increase longevity. Nor does it seem advisable in patients with stable although diminished cardiac capacity since frequently loss of mental acuity occurs following the procedure. Long-term changes to behavior, emphasizing diet and exercise plus a medicine regime tailored to lower blood pressure, lower cholesterol and lipids, and reduce clotting are equally as effective.
Chapter Review
The heart resides within the pericardial sac and is located in the mediastinal space within the thoracic cavity. The pericardial sac consists of two fused layers: an outer fibrous capsule and an inner parietal pericardium lined with a serous membrane. Between the pericardial sac and the heart is the pericardial cavity, which is filled with lubricating serous fluid. The walls of the heart are composed of an outer epicardium, a thick myocardium, and an inner lining layer of endocardium. The human heart consists of a pair of atria, which receive blood and pump it into a pair of ventricles, which pump blood into the vessels. The right atrium receives systemic blood relatively low in oxygen and pumps it into the right ventricle, which pumps it into the pulmonary circuit. Exchange of oxygen and carbon dioxide occurs in the lungs, and blood high in oxygen returns to the left atrium, which pumps blood into the left ventricle, which in turn pumps blood into the aorta and the remainder of the systemic circuit. The septa are the partitions that separate the chambers of the heart. They include the interatrial septum, the interventricular septum, and the atrioventricular septum. Two of these openings are guarded by the atrioventricular valves, the right tricuspid valve and the left mitral valve, which prevent the backflow of blood. Each is attached to chordae tendineae that extend to the papillary muscles, which are extensions of the myocardium, to prevent the valves from being blown back into the atria. The pulmonary valve is located at the base of the pulmonary trunk, and the left semilunar valve is located at the base of the aorta. The right and left coronary arteries are the first to branch off the aorta and arise from two of the three sinuses located near the base of the aorta and are generally located in the sulci. Cardiac veins parallel the small cardiac arteries and generally drain into the coronary sinus.
Interactive Link Questions
Visit this site to observe an echocardiogram of actual heart valves opening and closing. Although much of the heart has been “removed” from this gif loop so the chordae tendineae are not visible, why is their presence more critical for the atrioventricular valves (tricuspid and mitral) than the semilunar (aortic and pulmonary) valves?
Answer: The pressure gradient between the atria and the ventricles is much greater than that between the ventricles and the pulmonary trunk and aorta. Without the presence of the chordae tendineae and papillary muscles, the valves would be blown back (prolapsed) into the atria and blood would regurgitate.
Review Questions
Q. Which of the following is not important in preventing backflow of blood?
A. chordae tendineae
B. papillary muscles
C. AV valves
D. endocardium
Answer: D
Q. Which valve separates the left atrium from the left ventricle?
A. mitral
B. tricuspid
C. pulmonary
D. aortic
Answer: A
Q. Which of the following lists the valves in the order through which the blood flows from the vena cava through the heart?
A. tricuspid, pulmonary semilunar, bicuspid, aortic semilunar
B. mitral, pulmonary semilunar, bicuspid, aortic semilunar
C. aortic semilunar, pulmonary semilunar, tricuspid, bicuspid
D. bicuspid, aortic semilunar, tricuspid, pulmonary semilunar
Answer: A
Q. Which chamber initially receives blood from the systemic circuit?
A. left atrium
B. left ventricle
C. right atrium
D. right ventricle
Answer: C
Q. The ________ layer secretes chemicals that help to regulate ionic environments and strength of contraction and serve as powerful vasoconstrictors.
A. pericardial sac
B. endocardium
C. myocardium
D. epicardium
Answer: B
Q. The myocardium would be the thickest in the ________.
A. left atrium
B. left ventricle
C. right atrium
D. right ventricle
Answer: B
Q. In which septum is it normal to find openings in the adult?
A. interatrial septum
B. interventricular septum
C. atrioventricular septum
D. all of the above
Answer: C
Critical Thinking Questions
Q. Describe how the valves keep the blood moving in one direction.
A. When the ventricles contract and pressure begins to rise in the ventricles, there is an initial tendency for blood to flow back (regurgitate) to the atria. However, the papillary muscles also contract, placing tension on the chordae tendineae and holding the atrioventricular valves (tricuspid and mitral) in place to prevent the valves from prolapsing and being forced back into the atria. The semilunar valves (pulmonary and aortic) lack chordae tendineae and papillary muscles, but do not face the same pressure gradients as do the atrioventricular valves. As the ventricles relax and pressure drops within the ventricles, there is a tendency for the blood to flow backward. However, the valves, consisting of reinforced endothelium and connective tissue, fill with blood and seal off the opening preventing the return of blood.
Q. Why is the pressure in the pulmonary circulation lower than in the systemic circulation?
A. The pulmonary circuit consists of blood flowing to and from the lungs, whereas the systemic circuit carries blood to and from the entire body. The systemic circuit is far more extensive, consisting of far more vessels and offers much greater resistance to the flow of blood, so the heart must generate a higher pressure to overcome this resistance. This can be seen in the thickness of the myocardium in the ventricles.
Glossary
- anastomosis
- (plural = anastomoses) area where vessels unite to allow blood to circulate even if there may be partial blockage in another branch
- anterior cardiac veins
- vessels that parallel the small cardiac arteries and drain the anterior surface of the right ventricle; bypass the coronary sinus and drain directly into the right atrium
- anterior interventricular artery
- (also, left anterior descending artery or LAD) major branch of the left coronary artery that follows the anterior interventricular sulcus
- anterior interventricular sulcus
- sulcus located between the left and right ventricles on the anterior surface of the heart
- aortic valve
- (also, aortic semilunar valve) valve located at the base of the aorta
- atrioventricular septum
- cardiac septum located between the atria and ventricles; atrioventricular valves are located here
- atrioventricular valves
- one-way valves located between the atria and ventricles; the valve on the right is called the tricuspid valve, and the one on the left is the mitral or bicuspid valve
- atrium
- (plural = atria) upper or receiving chamber of the heart that pumps blood into the lower chambers just prior to their contraction; the right atrium receives blood from the systemic circuit that flows into the right ventricle; the left atrium receives blood from the pulmonary circuit that flows into the left ventricle
- auricle
- extension of an atrium visible on the superior surface of the heart
- bicuspid valve
- (also, mitral valve or left atrioventricular valve) valve located between the left atrium and ventricle; consists of two flaps of tissue
- cardiac notch
- depression in the medial surface of the inferior lobe of the left lung where the apex of the heart is located
- cardiac skeleton
- (also, skeleton of the heart) reinforced connective tissue located within the atrioventricular septum; includes four rings that surround the openings between the atria and ventricles, and the openings to the pulmonary trunk and aorta; the point of attachment for the heart valves
- cardiomyocyte
- muscle cell of the heart
- chordae tendineae
- string-like extensions of tough connective tissue that extend from the flaps of the atrioventricular valves to the papillary muscles
- circumflex artery
- branch of the left coronary artery that follows coronary sulcus
- coronary arteries
- branches of the ascending aorta that supply blood to the heart; the left coronary artery feeds the left side of the heart, the left atrium and ventricle, and the interventricular septum; the right coronary artery feeds the right atrium, portions of both ventricles, and the heart conduction system
- coronary sinus
- large, thin-walled vein on the posterior surface of the heart that lies within the atrioventricular sulcus and drains the heart myocardium directly into the right atrium
- coronary sulcus
- sulcus that marks the boundary between the atria and ventricles
- coronary veins
- vessels that drain the heart and generally parallel the large surface arteries
- endocardium
- innermost layer of the heart lining the heart chambers and heart valves; composed of endothelium reinforced with a thin layer of connective tissue that binds to the myocardium
- endothelium
- layer of smooth, simple squamous epithelium that lines the endocardium and blood vessels
- epicardial coronary arteries
- surface arteries of the heart that generally follow the sulci
- epicardium
- innermost layer of the serous pericardium and the outermost layer of the heart wall
- foramen ovale
- opening in the fetal heart that allows blood to flow directly from the right atrium to the left atrium, bypassing the fetal pulmonary circuit
- fossa ovalis
- oval-shaped depression in the interatrial septum that marks the former location of the foramen ovale
- great cardiac vein
- vessel that follows the interventricular sulcus on the anterior surface of the heart and flows along the coronary sulcus into the coronary sinus on the posterior surface; parallels the anterior interventricular artery and drains the areas supplied by this vessel
- hypertrophic cardiomyopathy
- pathological enlargement of the heart, generally for no known reason
- inferior vena cava
- large systemic vein that returns blood to the heart from the inferior portion of the body
- interatrial septum
- cardiac septum located between the two atria; contains the fossa ovalis after birth
- interventricular septum
- cardiac septum located between the two ventricles
- left atrioventricular valve
- (also, mitral valve or bicuspid valve) valve located between the left atrium and ventricle; consists of two flaps of tissue
- marginal arteries
- branches of the right coronary artery that supply blood to the superficial portions of the right ventricle
- mesothelium
- simple squamous epithelial portion of serous membranes, such as the superficial portion of the epicardium (the visceral pericardium) and the deepest portion of the pericardium (the parietal pericardium)
- middle cardiac vein
- vessel that parallels and drains the areas supplied by the posterior interventricular artery; drains into the great cardiac vein
- mitral valve
- (also, left atrioventricular valve or bicuspid valve) valve located between the left atrium and ventricle; consists of two flaps of tissue
- moderator band
- band of myocardium covered by endocardium that arises from the inferior portion of the interventricular septum in the right ventricle and crosses to the anterior papillary muscle; contains conductile fibers that carry electrical signals followed by contraction of the heart
- myocardium
- thickest layer of the heart composed of cardiac muscle cells built upon a framework of primarily collagenous fibers and blood vessels that supply it and the nervous fibers that help to regulate it
- papillary muscle
- extension of the myocardium in the ventricles to which the chordae tendineae attach
- pectinate muscles
- muscular ridges seen on the anterior surface of the right atrium
- pericardial cavity
- cavity surrounding the heart filled with a lubricating serous fluid that reduces friction as the heart contracts
- pericardial sac
- (also, pericardium) membrane that separates the heart from other mediastinal structures; consists of two distinct, fused sublayers: the fibrous pericardium and the parietal pericardium
- pericardium
- (also, pericardial sac) membrane that separates the heart from other mediastinal structures; consists of two distinct, fused sublayers: the fibrous pericardium and the parietal pericardium
- posterior cardiac vein
- vessel that parallels and drains the areas supplied by the marginal artery branch of the circumflex artery; drains into the great cardiac vein
- posterior interventricular artery
- (also, posterior descending artery) branch of the right coronary artery that runs along the posterior portion of the interventricular sulcus toward the apex of the heart and gives rise to branches that supply the interventricular septum and portions of both ventricles
- posterior interventricular sulcus
- sulcus located between the left and right ventricles on the anterior surface of the heart
- pulmonary arteries
- left and right branches of the pulmonary trunk that carry deoxygenated blood from the heart to each of the lungs
- pulmonary capillaries
- capillaries surrounding the alveoli of the lungs where gas exchange occurs: carbon dioxide exits the blood and oxygen enters
- pulmonary circuit
- blood flow to and from the lungs
- pulmonary trunk
- large arterial vessel that carries blood ejected from the right ventricle; divides into the left and right pulmonary arteries
- pulmonary valve
- (also, pulmonary semilunar valve, the pulmonic valve, or the right semilunar valve) valve at the base of the pulmonary trunk that prevents backflow of blood into the right ventricle; consists of three flaps
- pulmonary veins
- veins that carry highly oxygenated blood into the left atrium, which pumps the blood into the left ventricle, which in turn pumps oxygenated blood into the aorta and to the many branches of the systemic circuit
- right atrioventricular valve
- (also, tricuspid valve) valve located between the right atrium and ventricle; consists of three flaps of tissue
- semilunar valves
- valves located at the base of the pulmonary trunk and at the base of the aorta
- septum
- (plural = septa) walls or partitions that divide the heart into chambers
- septum primum
- flap of tissue in the fetus that covers the foramen ovale within a few seconds after birth
- small cardiac vein
- parallels the right coronary artery and drains blood from the posterior surfaces of the right atrium and ventricle; drains into the great cardiac vein
- sulcus
- (plural = sulci) fat-filled groove visible on the surface of the heart; coronary vessels are also located in these areas
- superior vena cava
- large systemic vein that returns blood to the heart from the superior portion of the body
- systemic circuit
- blood flow to and from virtually all of the tissues of the body
- trabeculae carneae
- ridges of muscle covered by endocardium located in the ventricles
- tricuspid valve
- term used most often in clinical settings for the right atrioventricular valve
- valve
- in the cardiovascular system, a specialized structure located within the heart or vessels that ensures one-way flow of blood
- ventricle
- one of the primary pumping chambers of the heart located in the lower portion of the heart; the left ventricle is the major pumping chamber on the lower left side of the heart that ejects blood into the systemic circuit via the aorta and receives blood from the left atrium; the right ventricle is the major pumping chamber on the lower right side of the heart that ejects blood into the pulmonary circuit via the pulmonary trunk and receives blood from the right atrium