
25.2: Anatomy ya jumla ya Usafiri wa Mkojo
- Page ID
- 178540

Malengo ya kujifunza
- Tambua ureters, kibofu cha mkojo, na urethra, pamoja na eneo lao, muundo, histology, na kazi
- Linganisha na kulinganisha urethra ya kiume na ya kike
- Eleza reflex micturition
- Eleza udhibiti wa hiari na usiohusika wa neural wa micturition
Badala ya kuanza na malezi ya mkojo, sehemu hii itaanza na excretion ya mkojo. Mkojo ni maji ya utungaji wa kutofautiana ambayo inahitaji miundo maalumu ili kuiondoa kutoka kwa mwili kwa usalama na kwa ufanisi. Damu inachujwa, na filtrate inabadilishwa kuwa mkojo kwa kiwango cha mara kwa mara siku nzima. Kioevu hiki kilichosindika kinahifadhiwa mpaka wakati unaofaa wa excretion. Miundo yote inayohusika katika usafiri na uhifadhi wa mkojo ni kubwa ya kutosha kuonekana kwa jicho la uchi. Mfumo huu wa usafiri na kuhifadhi sio tu maduka ya taka, lakini hulinda tishu kutokana na uharibifu kutokana na aina mbalimbali za pH na osmolarity ya mkojo, kuzuia maambukizi ya viumbe vya kigeni, na kwa kiume, hutoa kazi za uzazi.
Urethra
Urethra husafirisha mkojo kutoka kibofu cha kibofu hadi nje ya mwili ili uondoe. Urethra ni chombo pekee cha urologic kinachoonyesha tofauti yoyote muhimu ya anatomiki kati ya wanaume na wanawake; miundo mingine yote ya usafiri wa mkojo ni sawa (Kielelezo\(\PageIndex{1}\)).

Urethra katika wanaume na wanawake huanza duni na katikati ya fursa mbili za ureteral zinazounda pointi tatu za eneo la umbo la pembetatu chini ya kibofu cha kibofu kinachoitwa trigone (Kigiriki tri- = “pembetatu” na mzizi wa neno “trigonometry”). Urethra hufuatilia posterior na duni kwa symphysis ya pubic (angalia Mchoro\(\PageIndex{1}\) a.). Katika wanaume na wanawake, urethra ya kupakana imefungwa na epithelium ya mpito, wakati sehemu ya mwisho ni epithelium isiyo na keratinized, iliyokataliwa ya squamous. Katika kiume, epithelium ya pseudostratified columnar mistari urethra kati ya aina hizi mbili za seli. Voiding inasimamiwa na involuntary kujiendesha mfumo wa neva kudhibitiwa ndani ya mkojo sphincter, yenye misuli laini na hiari skeletal misuli ambayo hufanya nje ya mkojo sphincter chini yake.
Urethra ya kike
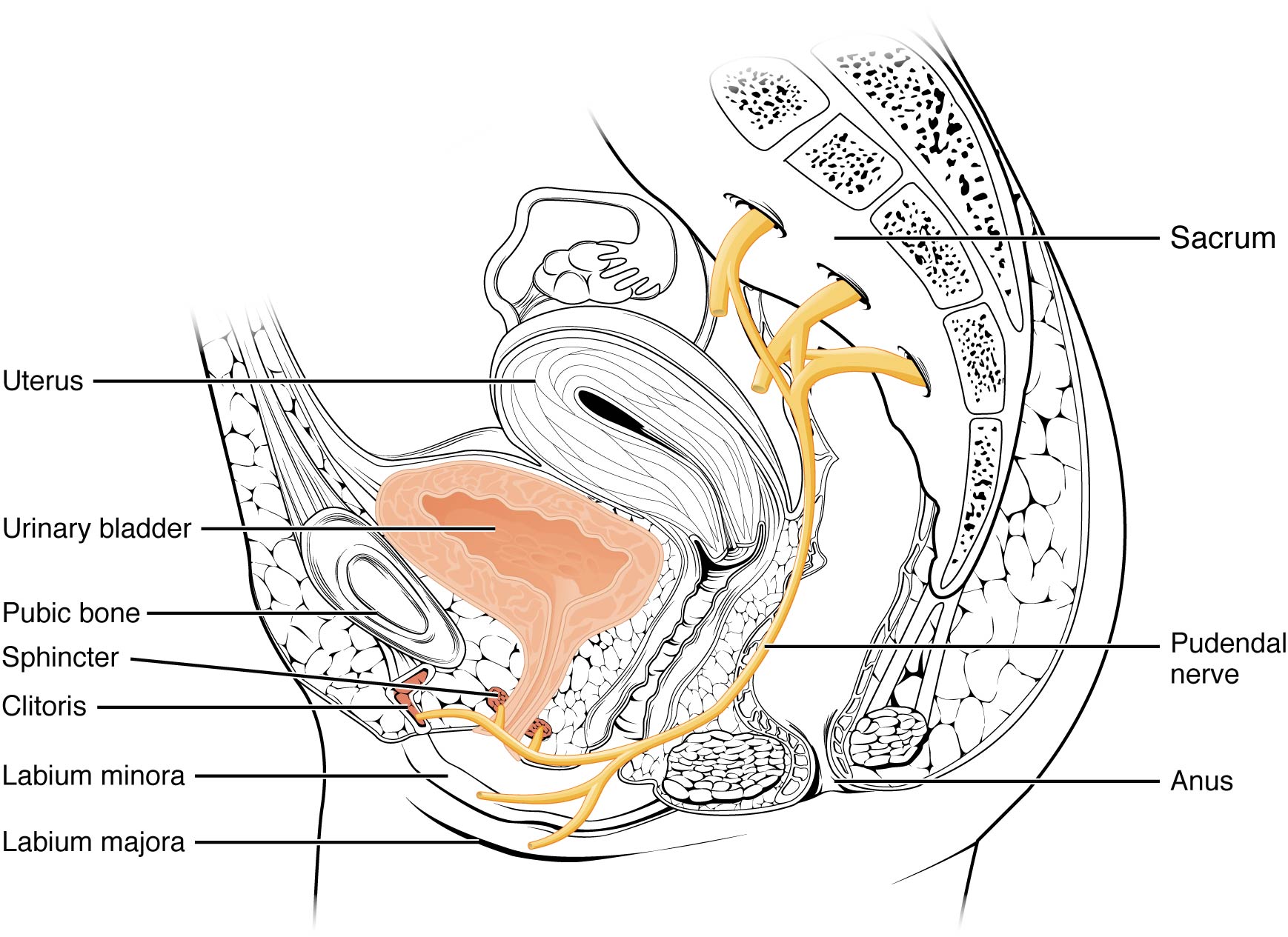
Orifice ya nje ya urethra imeingizwa kwenye ukuta wa uke wa anterior duni kuliko clitoris, bora kuliko ufunguzi wa uke (introitus), na medial kwa minora ya labia. Urefu wake mfupi, karibu 4 cm, ni chini ya kizuizi kwa bakteria ya fecal kuliko urethra ya kiume mrefu na maelezo bora kwa matukio makubwa ya UTI kwa wanawake. Udhibiti wa hiari wa sphincter ya nje ya urethra ni kazi ya ujasiri wa pudendal. Inatokea katika mkoa wa sacral wa kamba ya mgongo, kusafiri kupitia mishipa ya S2—S4 ya plexus ya sacral.
Urethra ya kiume
Urethra ya kiume hupita kupitia tezi ya prostate mara moja duni kwa kibofu cha kibofu kabla ya kupita chini ya symphysis ya pubic (angalia Mchoro\(\PageIndex{1}\) .b). Urefu wa urethra ya kiume hutofautiana kati ya wanaume lakini wastani wa cm 20 kwa urefu. Imegawanywa katika mikoa minne: urethra ya preprostatic, urethra ya prostatic, urethra ya membranous, na urethra ya spongy au ya penile. Urethra ya preprostatic ni mfupi sana na imeingizwa kwenye ukuta wa kibofu cha kibofu. Urethra ya prostatic hupita kupitia gland ya prostate. Wakati wa ngono, hupokea mbegu kupitia ducts ejaculatory na secretions kutoka vesicles seminal. Vipande vya Cowper vilivyooanishwa (tezi za bulbourethral) huzalisha na kuzalisha kamasi ndani ya urethra ili kuzuia pH ya urethra wakati wa kusisimua ngono. Kamasi haina neutralizes mazingira ya kawaida ya tindikali na husababisha urethra, kupunguza upinzani wa kumwagika. Urethra ya membranous hupita kupitia misuli ya kina ya perineum, ambako imewekeza na sphincters ya urethra inayozunguka. Urethra ya spongy hutoka kwenye ncha (orifice ya nje ya urethra) ya uume baada ya kupita kupitia spongiosum ya corpus. Vidonda vya mucous hupatikana pamoja na urefu wa urethra na kulinda urethra kutoka kwa kiasi kikubwa cha mkojo pH. Uhifadhi ni sawa katika wanaume na wanawake.
Kibofu
Kibofu cha mkojo hukusanya mkojo kutoka kwa ureters wote (Kielelezo\(\PageIndex{2}\)). Kibofu cha kibofu kiko anterior kwa uterasi kwa wanawake, baada ya mfupa wa pubic na anterior kwa rectum. Wakati wa ujauzito mwishoni, uwezo wake umepunguzwa kutokana na ukandamizaji na uterasi unaoenea, na kusababisha kuongezeka kwa mzunguko wa kukimbia. Katika wanaume, anatomy ni sawa, hupunguza uterasi, na kwa kuongeza ya prostate duni kwa kibofu cha kibofu. Kibofu cha mkojo ni sehemu ya retroperitoneal (nje ya cavity ya peritoneal) na “kuba” yake iliyofunikwa na peritoneal inayojitokeza ndani ya tumbo wakati kibofu cha mkojo kinapotoshwa na mkojo.
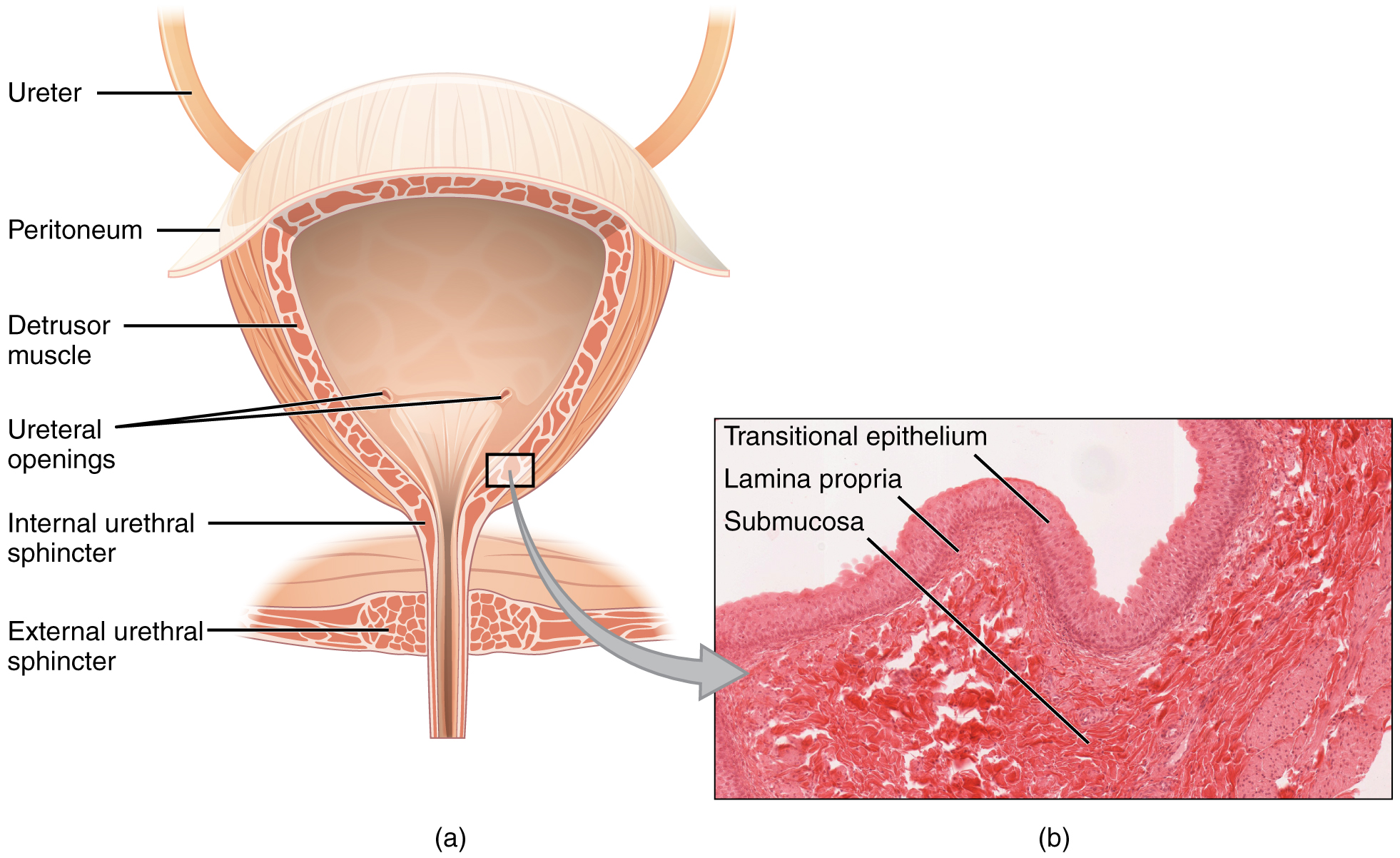

kibofu cha mkojo ni chombo distensible zikiwemo ya kawaida crisscrossing bendi ya misuli laini kwa pamoja aitwaye detrusor misuli. Uso wa mambo ya ndani unafanywa na epithelium ya seli ya mpito ambayo inafaa kwa mabadiliko makubwa ya kibofu cha kibofu. Wakati tupu, inafanana na epithelia ya columnar, lakini inapotambulishwa, “mabadiliko” (kwa hiyo jina) kwa kuonekana kwa squamous (angalia Mchoro\(\PageIndex{2}\)). Volumes in adults can range from nearly zero to 500–600 mL.
The detrusor muscle contracts with significant force in the young. The bladder’s strength diminishes with age, but voluntary contractions of abdominal skeletal muscles can increase intra-abdominal pressure to promote more forceful bladder emptying. Such voluntary contraction is also used in forceful defecation and childbirth.
Micturition Reflex
Micturition is a less-often used, but proper term for urination or voiding. It results from an interplay of involuntary and voluntary actions by the internal and external urethral sphincters. When bladder volume reaches about 150 mL, an urge to void is sensed but is easily overridden. Voluntary control of urination relies on consciously preventing relaxation of the external urethral sphincter to maintain urinary continence. As the bladder fills, subsequent urges become harder to ignore. Ultimately, voluntary constraint fails with resulting incontinence, which will occur as bladder volume approaches 300 to 400 mL.
Normal micturition is a result of stretch receptors in the bladder wall that transmit nerve impulses to the sacral region of the spinal cord to generate a spinal reflex. The resulting parasympathetic neural outflow causes contraction of the detrusor muscle and relaxation of the involuntary internal urethral sphincter. At the same time, the spinal cord inhibits somatic motor neurons, resulting in the relaxation of the skeletal muscle of the external urethral sphincter. The micturition reflex is active in infants but with maturity, children learn to override the reflex by asserting external sphincter control, thereby delaying voiding (potty training). This reflex may be preserved even in the face of spinal cord injury that results in paraplegia or quadriplegia. However, relaxation of the external sphincter may not be possible in all cases, and therefore, periodic catheterization may be necessary for bladder emptying.
Nerves involved in the control of urination include the hypogastric, pelvic, and pudendal (Figure \(\PageIndex{3}\)). Voluntary micturition requires an intact spinal cord and functional pudendal nerve arising from the sacral micturition center. Since the external urinary sphincter is voluntary skeletal muscle, actions by cholinergic neurons maintain contraction (and thereby continence) during filling of the bladder. At the same time, sympathetic nervous activity via the hypogastric nerves suppresses contraction of the detrusor muscle. With further bladder stretch, afferent signals traveling over sacral pelvic nerves activate parasympathetic neurons. This activates efferent neurons to release acetylcholine at the neuromuscular junctions, producing detrusor contraction and bladder emptying.
Ureters
The kidneys and ureters are completely retroperitoneal, and the bladder has a peritoneal covering only over the dome. As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel-shaped renal pelvis in the hilum of each kidney. The hilum narrows to become the ureter of each kidney. As urine passes through the ureter, it does not passively drain into the bladder but rather is propelled by waves of peristalsis. As the ureters enter the pelvis, they sweep laterally, hugging the pelvic walls. As they approach the bladder, they turn medially and pierce the bladder wall obliquely. This is important because it creates an one-way valve (a physiological sphincter rather than an anatomical sphincter) that allows urine into the bladder but prevents reflux of urine from the bladder back into the ureter. Children born lacking this oblique course of the ureter through the bladder wall are susceptible to “vesicoureteral reflux,” which dramatically increases their risk of serious UTI. Pregnancy also increases the likelihood of reflux and UTI.
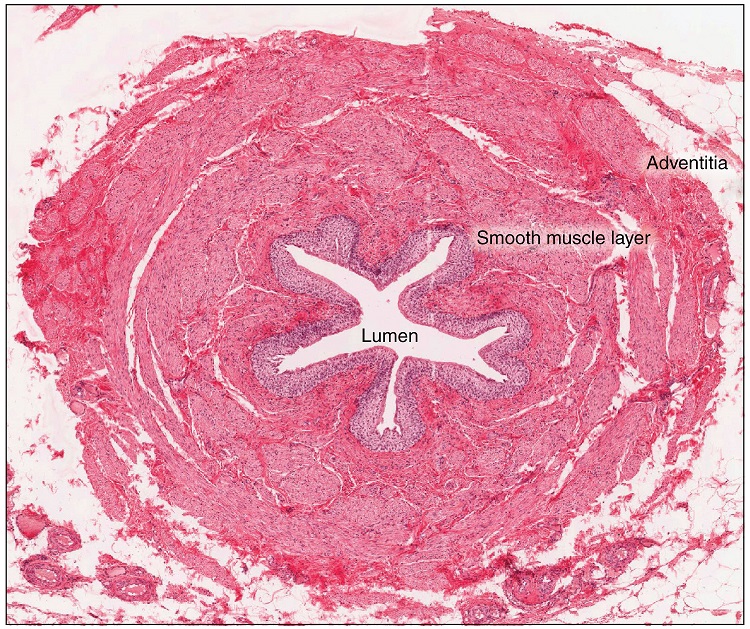
The ureters are approximately 30 cm long. The inner mucosa is lined with transitional epithelium (Figure \(\PageIndex{4}\)) and scattered goblet cells that secrete protective mucus. The muscular layer of the ureter consists of longitudinal and circular smooth muscles that create the peristaltic contractions to move the urine into the bladder without the aid of gravity. Finally, a loose adventitial layer composed of collagen and fat anchors the ureters between the parietal peritoneum and the posterior abdominal wall.
Chapter Review
The urethra is the only urinary structure that differs significantly between males and females. This is due to the dual role of the male urethra in transporting both urine and semen. The urethra arises from the trigone area at the base of the bladder. Urination is controlled by an involuntary internal sphincter of smooth muscle and a voluntary external sphincter of skeletal muscle. The shorter female urethra contributes to the higher incidence of bladder infections in females. The male urethra receives secretions from the prostate gland, Cowper’s gland, and seminal vesicles as well as sperm. The bladder is largely retroperitoneal and can hold up to 500–600 mL urine. Micturition is the process of voiding the urine and involves both involuntary and voluntary actions. Voluntary control of micturition requires a mature and intact sacral micturition center. It also requires an intact spinal cord. Loss of control of micturition is called incontinence and results in voiding when the bladder contains about 250 mL urine. The ureters are retroperitoneal and lead from the renal pelvis of the kidney to the trigone area at the base of the bladder. A thick muscular wall consisting of longitudinal and circular smooth muscle helps move urine toward the bladder by way of peristaltic contractions.
Review Questions
Q. Peristaltic contractions occur in the ________.
A. urethra
B. bladder
C. ureters
D. urethra, bladder, and ureters
Answer: C
Q. Somatic motor neurons must be ________ to relax the external urethral sphincter to allow urination.
A. stimulated
B. inhibited
Answer: B
Q. Which part of the urinary system is not completely retroperitoneal?
A. kidneys
B. ureters
C. bladder
D. nephrons
Answer: C
Critical Thinking Questions
Q. Why are females more likely to contract bladder infections than males?
A. The longer urethra of males means bacteria must travel farther to the bladder to cause an infection.
Q. Describe how forceful urination is accomplished.
A. Forceful urination is accomplished by contraction of abdominal muscles.
Glossary
- anatomical sphincter
- smooth or skeletal muscle surrounding the lumen of a vessel or hollow organ that can restrict flow when contracted
- detrusor muscle
- smooth muscle in the bladder wall; fibers run in all directions to reduce the size of the organ when emptying it of urine
- external urinary sphincter
- skeletal muscle; must be relaxed consciously to void urine
- internal urinary sphincter
- smooth muscle at the juncture of the bladder and urethra; relaxes as the bladder fills to allow urine into the urethra
- incontinence
- loss of ability to control micturition
- micturition
- also called urination or voiding
- physiological sphincter
- sphincter consisting of circular smooth muscle indistinguishable from adjacent muscle but possessing differential innervations, permitting its function as a sphincter; structurally weak
- retroperitoneal
- outside the peritoneal cavity; in the case of the kidney and ureters, between the parietal peritoneum and the abdominal wall
- sacral micturition center
- group of neurons in the sacral region of the spinal cord that controls urination; acts reflexively unless its action is modified by higher brain centers to allow voluntary urination
- trigone
- area at the base of the bladder marked by the two ureters in the posterior–lateral aspect and the urethral orifice in the anterior aspect oriented like points on a triangle
- urethra
- transports urine from the bladder to the outside environment